Pulmonary hemorrhage as an unusual initial manifestation of systemic lupus erythematosus
- Affiliations
-
- 1Department of Pediatrics, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea. jy7.shim@samsung.com
- KMID: 2218649
- DOI: http://doi.org/10.4168/aard.2015.3.5.370
Abstract
- Pulmonary hemorrhage as the initial manifestation of systemic lupus erythematosus (SLE) has been rarely reported in children. We present the case of a 10-year-old girl who was admitted to Kangbuk Samsung Hospital with hemoptysis. She had a 5-day history of cough with dyspnea. On physical exam, breath sound was significantly decreased combined with rales on both lung fields. Blood tests revealed pancytopenia, decreased complement levels (C3, 21.28 mg/dL; C4, 3.10 mg/dL), positive antinuclear antibody (>1:640) and anti-double-stranded DNA antibody (262.5 IU/mL). Chest computed tomography revealed patchy ground glass opacity on both lung fields. She had proteinuria and diffuse lupus nephritis (International Society of Nephrology/Renal Pathology Society class IV-G(A)) confirmed by renal biopsy. High-dose methylprednisolone pulse therapy (30 mg/kg/day) was given for 3 days and then switched to a maintenance dose (1 mg/kg/day). Initially hemoptysis resolved after administration of methylprednisolone, but recurred on the 14th day of treatment. She was then treated with cyclophosphamide pulse therapy and hemoptysis subsided without recurrence. She was discharged on the 31st day of admission. She continued to receive monthly cyclophosphamide pulse therapy until the occurrence of leukopenia and then her regimen was switched to mycophenolate and hydroxychloroquine. SLE continues to be well controlled after 18 months of treatment. Recognition of pulmonary hemorrhage as a possible initial manifestation of SLE is crucial for early diagnosis. SLE was successfully treated with good outcome.
MeSH Terms
-
Antibodies, Antinuclear
Biopsy
Child
Complement System Proteins
Cough
Cyclophosphamide
DNA
Dyspnea
Early Diagnosis
Female
Glass
Hematologic Tests
Hemoptysis
Hemorrhage*
Humans
Hydroxychloroquine
Leukopenia
Lung
Lupus Erythematosus, Systemic*
Lupus Nephritis
Methylprednisolone
Pancytopenia
Pathology
Pediatrics
Proteinuria
Recurrence
Respiratory Sounds
Thorax
Antibodies, Antinuclear
Complement System Proteins
Cyclophosphamide
DNA
Hydroxychloroquine
Methylprednisolone
Figure
-

Fig. 1 Chest radiograph at admission (A), at hospital day 20th (B), at discharge (C). (A) Initial chest radiograph shows diffuse ground glass opacities and consolidations in both lung fields. (B) Twenty days later, bilateral ground glass opacities are extended. (C) Previous ground glass opacities are nearly disappeared in both lung fields.
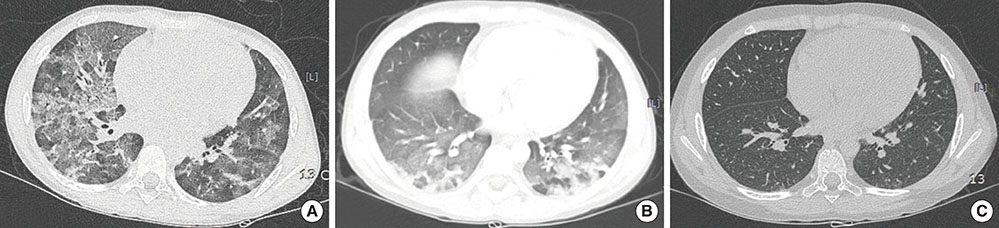
Fig. 2 Computed tomography image at 2nd day (A), at 21st day (B), and at discharge (C). (A) Axial computed tomography image demonstrates diffuse bilateral ground glass opacities with interlobular and intralobular septal line thickening. (B) Previous bilateral ground glass opacities are decreased in the both lung fields, but there are newly developed multifocal ground glass opacities and consolidations at superior segment of both lower lobes. (C) Previous ground glass opacities are disappeared at both lung fields.

Fig. 3 An overview of clinical course associated with treatment modality. HD, hospital day; O2, oxygen; C3, complement component 3.
Reference
-
1. Mok CC, Lau CS. Pathogenesis of systemic lupus erythematosus. J Clin Pathol. 2003; 56:481–490.
Article2. Cervera R, Khamashta MA, Font J, Sebastiani GD, Gil A, Lavilla P, et al. Morbidity and mortality in systemic lupus erythematosus during a 10-year period: a comparison of early and late manifestations in a cohort of 1,000 patients. Medicine (Baltimore). 2003; 82:299–308.
Article3. Santos-Ocampo AS, Mandell BF, Fessler BJ. Alveolar hemorrhage in systemic lupus erythematosus: presentation and management. Chest. 2000; 118:1083–1090.
Article4. Ciftci E, Yalcinkaya F, Ince E, Ekim M, Ileri M, Orgerin Z, et al. Pulmonary involvement in childhood-onset systemic lupus erythematosus: a report of five cases. Rheumatology (Oxford). 2004; 43:587–591.
Article5. Bader-Meunier B, Armengaud JB, Haddad E, Salomon R, Deschenes G, Kone-Paut I, et al. Initial presentation of childhood-onset systemic lupus erythematosus: a French multicenter study. J Pediatr. 2005; 146:648–653.
Article6. Uziel Y, Laxer RM, Silverman ED. Persistent pulmonary hemorrhage as the sole initial clinical manifestation of pediatric systemic lupus erythematosus. Clin Exp Rheumatol. 1997; 15:697–700.7. Miller RW, Salcedo JR, Fink RJ, Murphy TM, Magilavy DB. Pulmonary hemorrhage in pediatric patients with systemic lupus erythematosus. J Pediatr. 1986; 108:576–579.
Article8. Weening JJ, D'Agati VD, Schwartz MM, Seshan SV, Alpers CE, Appel GB, et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004; 65:521–530.
Article9. Hiraki LT, Benseler SM, Tyrrell PN, Hebert D, Harvey E, Silverman ED. Clinical and laboratory characteristics and long-term outcome of pediatric systemic lupus erythematosus: a longitudinal study. J Pediatr. 2008; 152:550–556.
Article10. Eagen JW, Memoli VA, Roberts JL, Matthew GR, Schwartz MM, Lewis EJ. Pulmonary hemorrhage in systemic lupus erythematosus. Medicine (Baltimore). 1978; 57:545–560.
Article11. Belmont HM, Abramson SB, Lie JT. Pathology and pathogenesis of vascular injury in systemic lupus erythematosus. Interactions of inflammatory cells and activated endothelium. Arthritis Rheum. 1996; 39:9–22.
Article12. Bidwell JL, Pachner RW. Hemoptysis: diagnosis and management. Am Fam Physician. 2005; 72:1253–1260.13. Samad AS, Lindsley CB. Treatment of pulmonary hemorrhage in childhood systemic lupus erythematosus with mycophenolate mofetil. South Med J. 2003; 96:705–707.
Article14. Ruiz-Irastorza G, Ramos-Casals M, Brito-Zeron P, Khamashta MA. Clinical efficacy and side effects of antimalarials in systemic lupus erythematosus: a systematic review. Ann Rheum Dis. 2010; 69:20–28.
Article15. Austin HA 3rd, Klippel JH, Balow JE, le Riche NG, Steinberg AD, Plotz PH, et al. Therapy of lupus nephritis. Controlled trial of prednisone and cytotoxic drugs. N Engl J Med. 1986; 314:614–619.16. Hahn BH, McMahon MA, Wilkinson A, Wallace WD, Daikh DI, Fitzgerald JD, et al. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res (Hoboken). 2012; 64:797–808.
Article17. Bertsias GK, Tektonidou M, Amoura Z, Aringer M, Bajema I, Berden JH, et al. Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann Rheum Dis. 2012; 71:1771–1782.
Article18. Paredes A. Can mycophenolate mofetil substitute cyclophosphamide treatment of pediatric lupus nephritis? Pediatr Nephrol. 2007; 22:1077–1082.
Article19. Bagga A, Hari P, Moudgil A, Jordan SC. Mycophenolate mofetil and prednisolone therapy in children with steroid-dependent nephrotic syndrome. Am J Kidney Dis. 2003; 42:1114–1120.
Article20. Marks SD, Tullus K. Modern therapeutic strategies for paediatric systemic lupus erythematosus and lupus nephritis. Acta Paediatr. 2010; 99:967–974.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Hemorrhage with Hemoptysis in Systemic Lupus Erythematosis
- A Case of Transverse Myelitis as a First Manifestation of Systemic Lupus Erythematosus
- Two Cases of Pulmonary Problems as Initial Clinical Manifestations of Systemic Lupus Erythematosus
- Cardiac tamponade as an initial manifestation of systemic lupus erythematosus--single case report
- A Case of Steroid-responsive Pericardial Effusion as an Initial Manifestation of Childhood Systemic Lupus Erythematosus
