A Case of Idiopathic Pediatric Acute Branch Retinal Artery Occlusion Involving the Macular Area
- Affiliations
-
- 1Department of Ophthalmology, Daegu Fatima Hospital, Daegu, Korea. mjmom99@naver.com
- KMID: 2218428
- DOI: http://doi.org/10.3341/jkos.2014.55.2.304
Abstract
- PURPOSE
We report a case of branch retinal artery occlusion (BRAO) interconnected with the perifoveal capillaries in a healthy young female.
CASE SUMMARY
A 16-year-old female presented with sudden loss of vision in her left eye. Upon initial examination, her left visual acuity was 0.02 and intraocular pressure was 31 mm Hg. Fundus examination revealed pallid retinal edema of the inferior posterior pole and retinal hemorrhage below optic disc. Ocular massage followed by anterior chamber paracentesis was performed for 30 minutes within 4 hours after the onset of vision loss. Fluorescein angiography (FAG) showed a very slow blood flow in the superotemporal and inferotemporal retinal arteries and a delay in retinal arteriovenous transit time. We performed hemodynamic tests such as blood pressure, echocardiography, and the hematologic test for thrombogenicity and all tests were normal. At three weeks after treatment, vision in the left eye was 0.7 and FAG revealed normal retinal arterial circulation and venous drainage time.
CONCLUSIONS
This is the first report regarding acute BRAO in a healthy Korean child without any detectable systemic disorder. Prompt treatment can prevent permanent visual loss in BRAO involving the macular area.
MeSH Terms
Figure
-
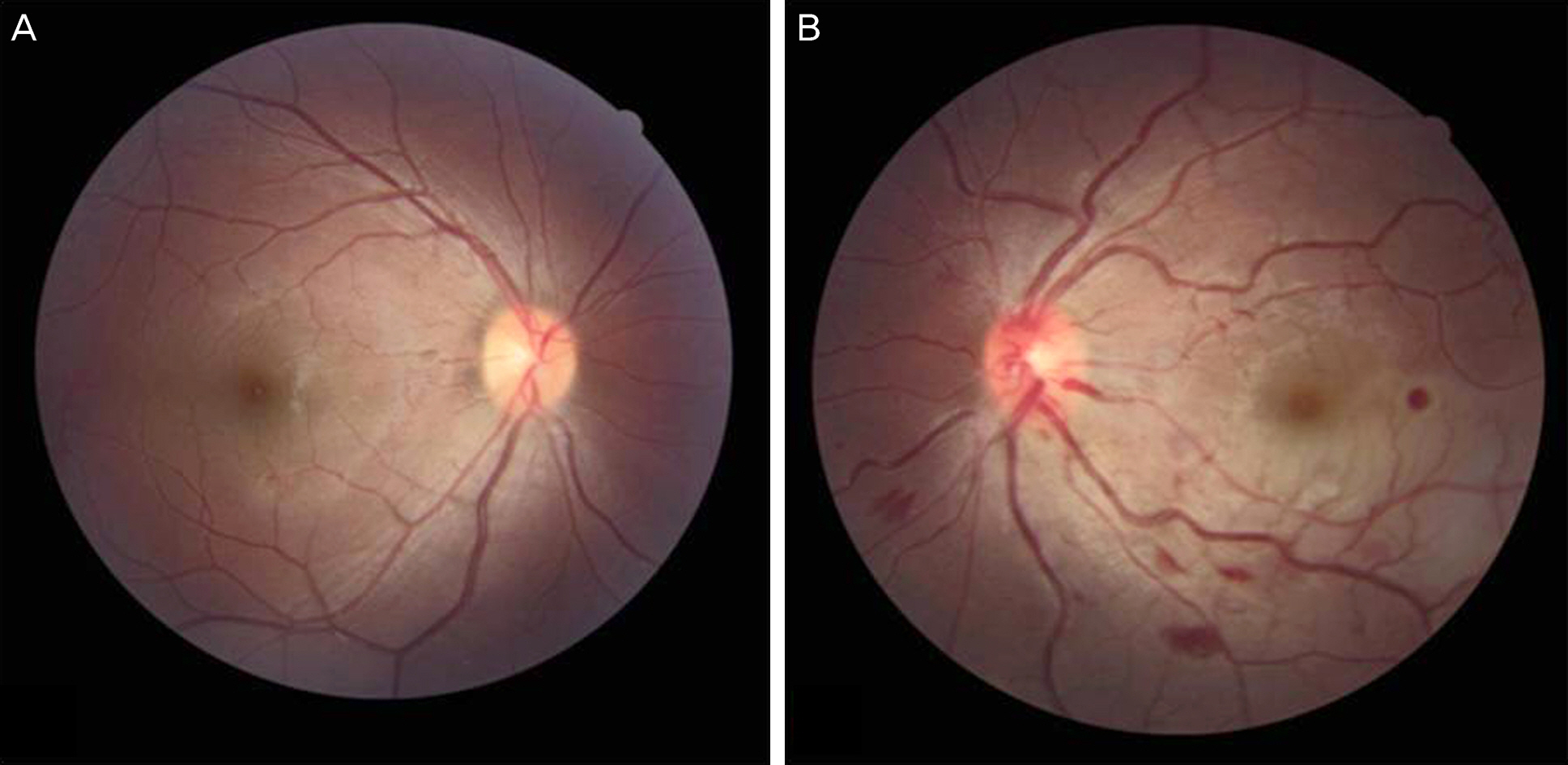
Figure 1. Color fundus photography of the right eye shows a normal retina (A), a pale retina along the inferotemporal vascular arcade, mild venous tortuosity, and flame shaped retinal hemorrhages are seen in the left eye (B).
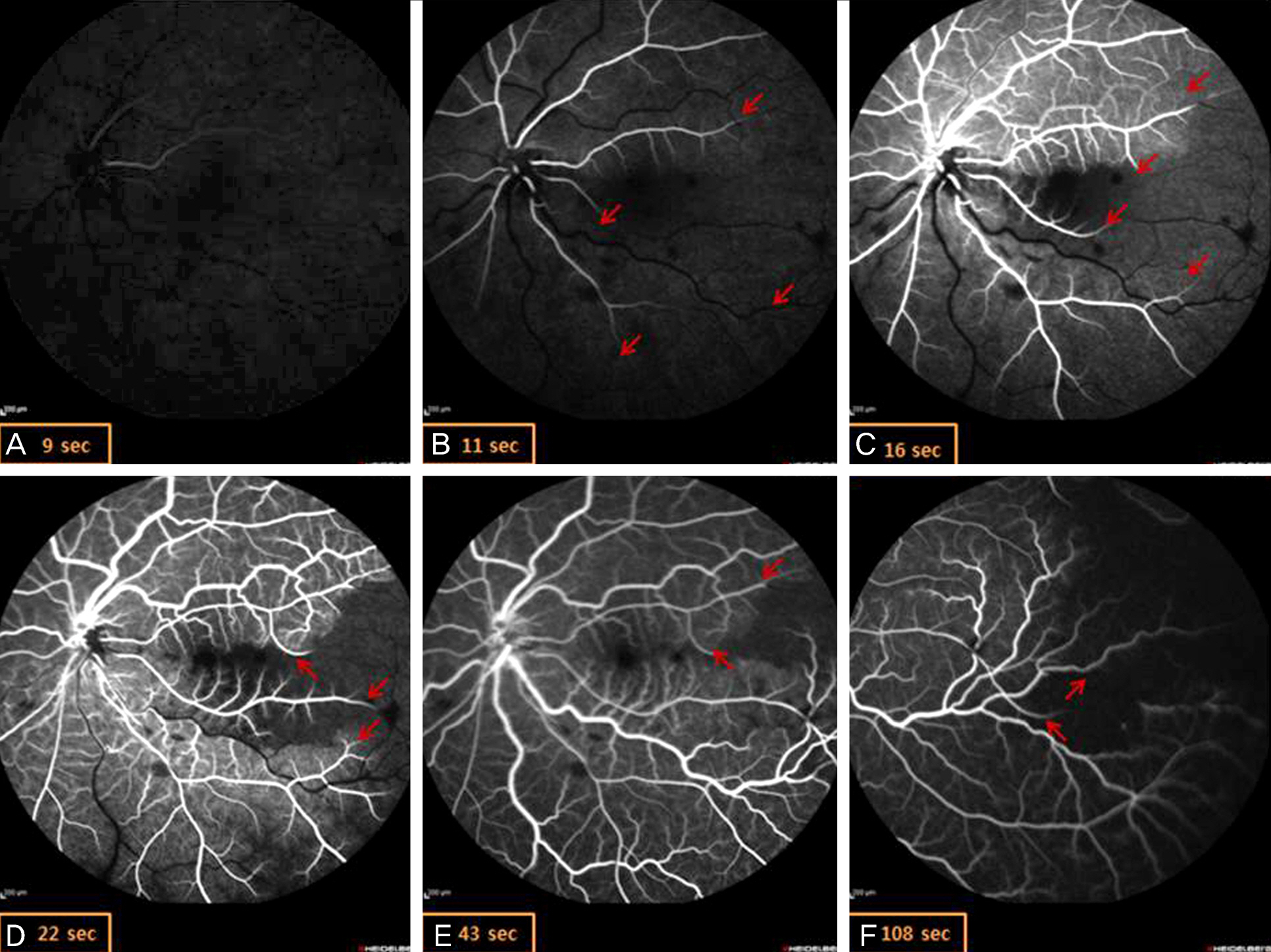
Figure 2. Fluorescent angiography of the left eye after ocular massage. Superotemporal and inferotemporal branch retinal arteries filling is very delayed, whereas the choroidal vascular bed fills normally. Ateriovenous transit time (E-B) is delayed to about 32 seconds. Dye is reached to temporal peripheral area for 2 minutes. Red arrows show the sites of the downstream filling defects.
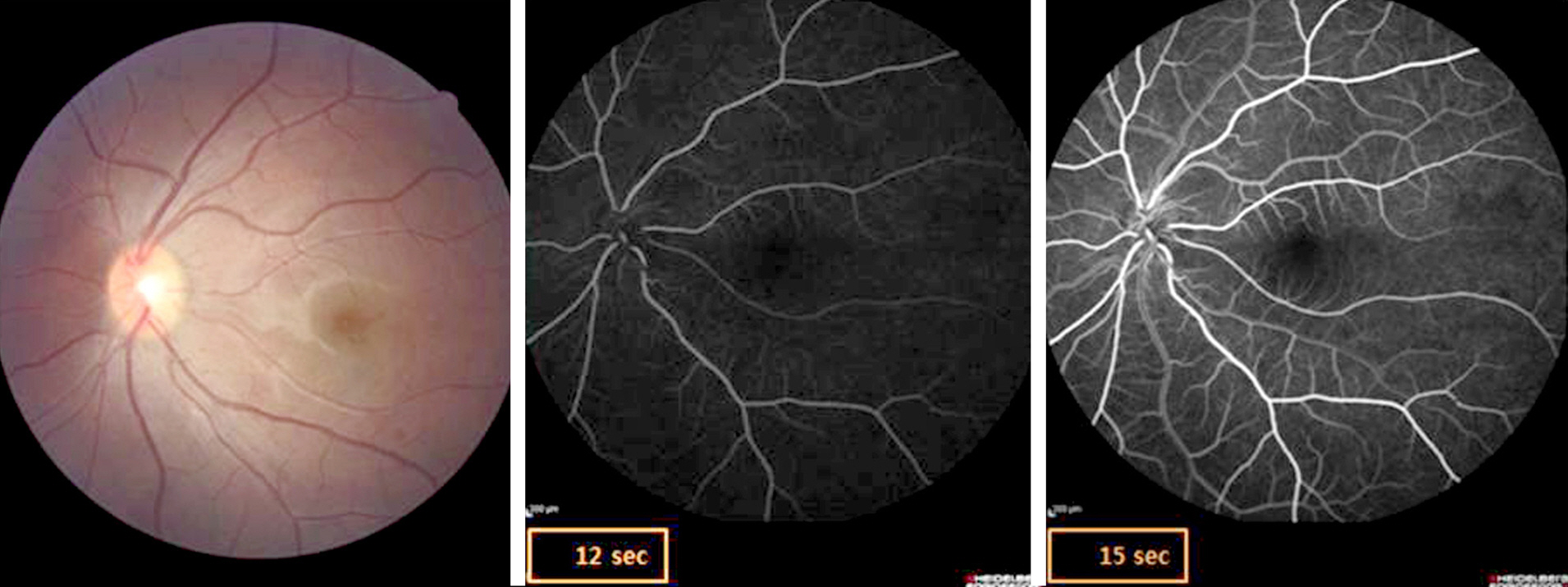
Figure 3. Color fundus photography and fluorescent angiography of the left eye 3 weeks after treatment. Arterial filling and arteriovenous transit time is normal. There is no retinal arterial occlusion.
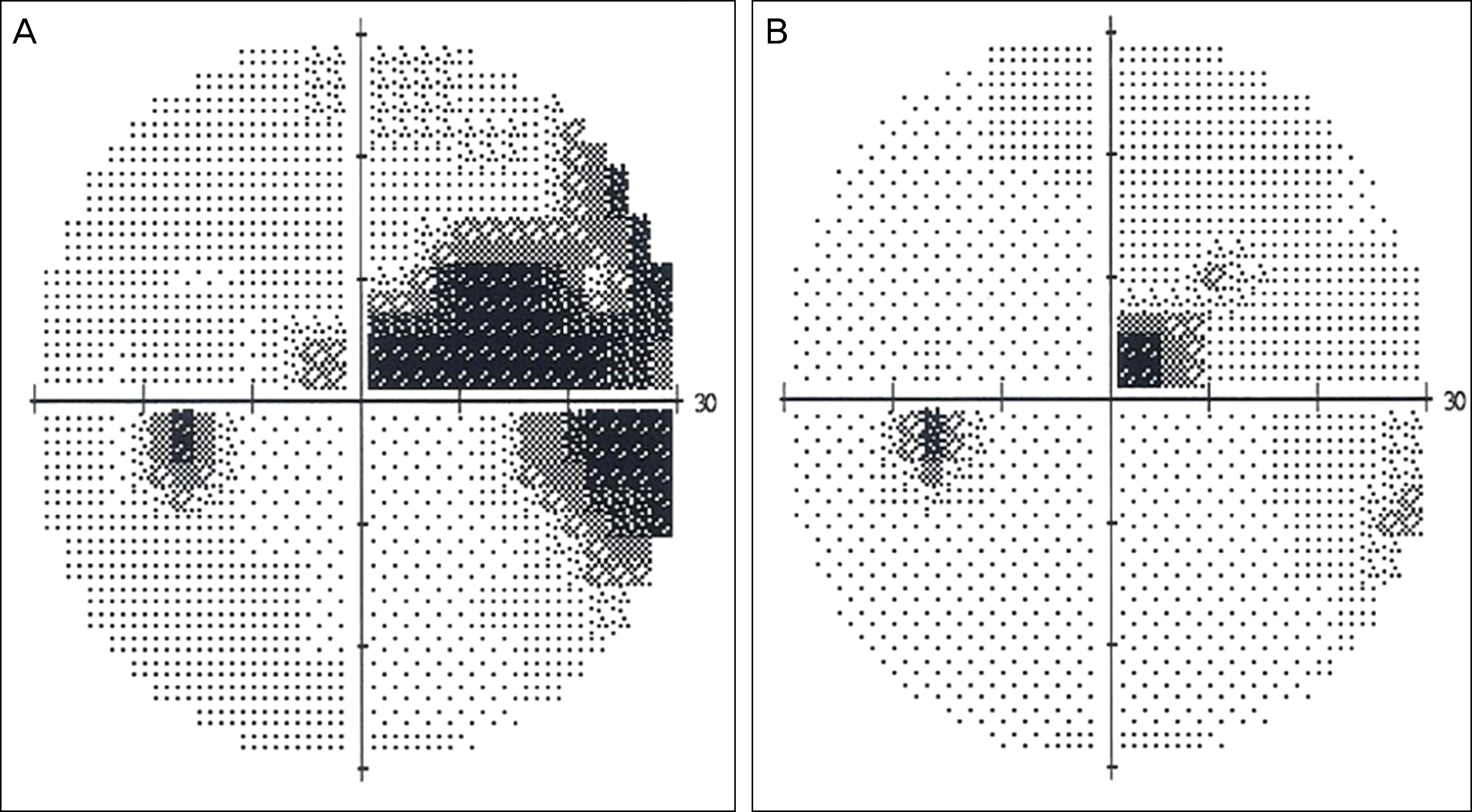
Figure 4. Visual field examination of the left eye (A) at initial examination, (B) at 3 weeks after treatment. Visual field reveals slight superior central scotoma within 10 degrees.
Reference
-
References
1. Brown GC, Magargal LE, Shields JA. . Retinal arterial obstruction in children and young adults. Ophthalmology. 1981; 88:18–25.
Article2. Greven CM, Slusher MM, Weaver RG.Retinal arterial occlusions in young adults. Am J Ophthalmol. 1995; 120:776–83.
Article3. Ratra D, Dhupper M.Retinal arterial occlusions in the young: sys-temic associations in Indian population. Indian J Ophthalmol. 2012; 60:95–100.
Article4. Manayath GJ, Shah PK, Narendran V, Morris RJ.Idiopathic pedia-tric retinal artery occlusion. Indian J Ophthalmol. 2010; 58:151–2.
Article5. Ros MA, Magargal LE, Uram M.Branch retinal-artery obstruction: a review of 201 eyes. Ann Ophthalmol. 1989; 21:103–7.6. Keyser BJ, Duker JS, Brown GC. . Combined central retinal vein occlusion and cilioretinal artery occlusion associated with prolonged retinal arterial filling. Am J Ophthalmol. 1994; 117:308–13.7. Hayreh SS, Podhajsky PA, Zimmerman MB.Branch retinal artery occlusion: natural history of visual outcome. Ophthalmology. 2009; 116:1188–94.e1-4.8. Lim JY, Lee JY, Chung HW. . Treatment of branch retinal ar-tery occlusion with transluminal Nd:YAG laser embolysis. Korean J Ophthalmol. 2009; 23:315–7.
Article9. Cugati S, Varma DD, Chen CS, Lee AW.Treatment options for central retinal artery occlusion. Curr Treat Options Neurol. 2013; 15:63–77.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Retinal Arteriolar Changes in a Patient with Branch Retinal Vein Occlusion
- The Macular Circulation State on BRVO According to Occlusion Site
- Clinical Features According to the Occlusion Site in Patients with Branch Retinal Vein Occlusion
- Clinical Aspect of Branch Retinal Vein Occlusion
- Central Retinal Artery Occlusion Masquerading as Branch Retinal Artery Occlusion
