A Case of Unilateral Electric Cataract with Optic Neuropathy after Electric Injury
- Affiliations
-
- 1Department of Ophthalmology, Maryknoll Hospital, Busan, Korea. pearlsj@hanmail.net
- 2Department of Ophthalmology, Haeundae Paek Hospital, Inje University College of Medicine, Busan, Korea.
- KMID: 2216955
- DOI: http://doi.org/10.3341/jkos.2013.54.4.680
Abstract
- PURPOSE
Electric injury may result in cataracts, which usually occur bilaterally. In this report, we present a rare complication of such an injury presenting as a unilateral cataract with optic neuropathy.
CASE SUMMARY
A 17-year-old male patient presented with gradual worsening of vision in his right eye 7 weeks after sustaining an injury from 22,900 volts of high-voltage electric current his right hand. On initial eye examination, the best corrected visual acuity (BCVA) was 20/60 in the right eye and 20/20 in the left eye. Relative afferent pupillary defect (RAPD) was noted in the right eye. Slit-lamp examination confirmed the typical anterior subcapsular lenticular opacities and funduscopy showed a slightly pale optic nerve head in the right eye. Pattern reversal visually evoked potential (P-VEP) showed a significant delay of P-100 implicit time in the right eye. After 7 months, phacoaspiration and posterior chamber intraocular lens implantation were performed in the right eye. Postoperatively, the BCVA improved to 20/30 but visual field examination showed a partial defect in the temporal area of the right eye. Cataract did not develop in the left eye during 15 months of follow-up. The electron microscopic findings showed that the number of mitochondria in the cytoplasm increased. The rough endoplasmic reticulum in the cytoplasm and microfilaments were enriched.
CONCLUSIONS
Manifestation time of ocular complications after electric injuries is different. Therefore an ophthalmic examination should be performed regularly in the early recovery period of such injuries and in particular, progression of bilateral electric cataract must be checked.
MeSH Terms
Figure
-
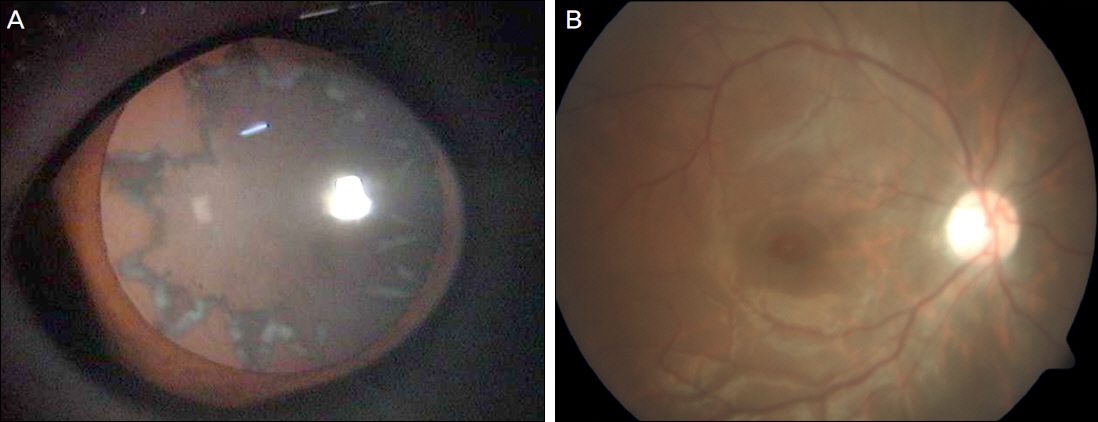
Figure 1. (A) Preoperative slit lamp examination photograph shows an anterior subcapsular radial shape-like opacities in the right eye 7 weeks after electrical injury. (B) Funduscopy photograph shows a blurred fundus, mild pale optic disc and about 0.3 of C/D ratio in the right eye.
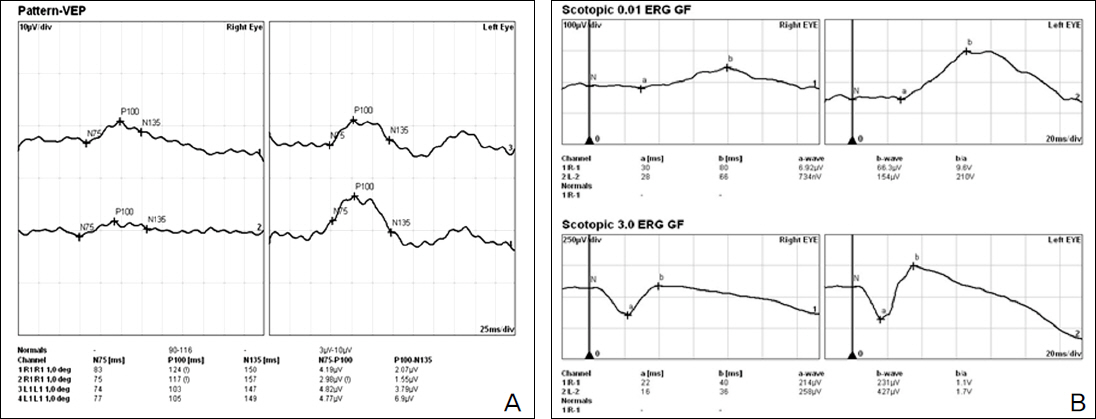
Figure 2. (A) Pattern reversal visually evoked potential (P-VEP) showed a significant delay of P100 latency and decrease of amplitude in the right eye. (B) Electroretinogram (ERG) shows decreased b-wave amplitude in the right eye.
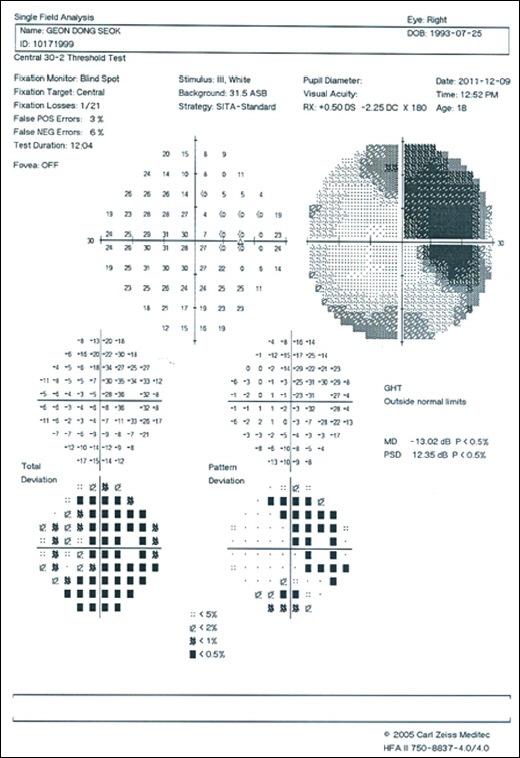
Figure 3. Thumbnail of Humphrey visual field examination shows a temporal area defect in the right eye.
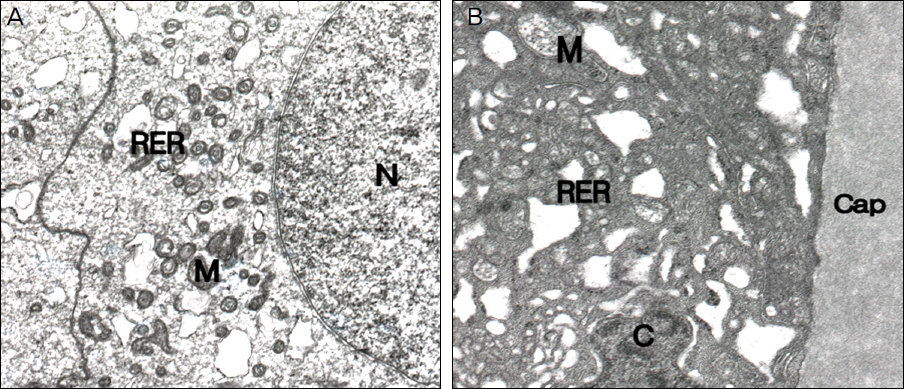
Figure 4. Electron micrograph of lens epithelial cell shows a pathologic findings of electrical cataract. (A) The number of mitochondria (M) in the cytoplasm is increased. The rough endoplasmic reticulum (RER) in the cytoplasm is dilated (×;8,000). (B) Interface between the capsule (Cap) and lens epithelial cell is well preserved. Nucleus chromatin (C) clumping was slightly increased and oval shaped mitochondria (M) are presented (×;12,000).
Reference
-
References
1. Han JR, Park IW. The clinical evaluation of ocular complications from electrical burn injury. J Korean Ophthalmol Soc. 2004; 45:281–6.2. Fraunfelder F, Hampton R. Electrical injury Current ocular therapy. 3rd ed.WB Saunders Co.;1990. p. 320–7.3. Solem L, Fischer RP, Strate RG. The natural history of electrical injury. J Trauma. 1977; 17:487–92.
Article4. Luce EA. Electrical burns. Clin Plast Surg. 2000; 27:133–43.
Article5. Boozalis GT, Purdue GF, Hunt JL, McCulley JP. Ocular changes Korean Ophthalmol Soc. 1980; 21:201–3.9. Park BI, Huh W. A case of electric cataract. J Korean Ophthalmol Soc. 1985; 26:799–801.10. Duke-Elder S. System of ophthalmology. 14. St. Louis: CV Mosby Co.;1972. p. 828–35.11. Long JC. A clinical and experimental study of electric cataract. Trans Am Ophthalmol Soc. 1962; 60:471–516.12. Bellows JG, Chinn H. Pathogenesis of electric cataract. Arch Ophthalmol. 1941; 26:606–12.13. von Bahr G.Electrical injuries. Ophthalmologica. 1969; 1-3:109–17.
Article14. Archer DB. Dermot Pierse lecture. Injuries of the posterior segment of the eye. Trans Ophthalmol Soc U K. 1985; 104(Pt 6):597–615.15. Kim YJ, Ahn SK, Shyn KH. Electron microscopic findings of the cataractous lens epithelium. J Korean Ophthalmol Soc. 1994; 35:263–70.16. Matsuura H. Electron microscopic observations in human senile and anterior polar cataract. Yonago Acta Med. 1968; 12:75–80.17. Vasavada AR, Cherian M, Yadav S, Rawal UM. Lens epithelial cell density and histomorphological study in cataractous lenses. J Cataract Refract Surg. 1991; 17:798–804.
Article18. Straatsma BR, Lightfoot DO, Barke RM, Horwitz J. Lens capsule and epithelium in age-related cataract. Am J Ophthalmol. 1991; 112:283–96.
Article19. Hanna C, Fraunfelder FT. Electric cataracts. II. Ultrastructural lens changes. Arch Ophthalmol. 1972; 87:184–91.
Article20. Yoon JW, Song BJ, Choi YI. Ultrastructure of the lens epithelium in two cases of the electric cataract. J Korean Ophthalmol Soc. 1998; 39:2938–45.
