A Case of Alkali Burn Treated With Amniotic Membrane Graft and Forniceal Reconstruction
- Affiliations
-
- 1Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea.
- 2Seoul Artificial Eye Center, Seoul National University Hospital Clinical Research Institute, Seoul, Korea.
- 3Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2213792
- DOI: http://doi.org/10.3341/jkos.2010.51.7.1010
Abstract
- PURPOSE
To report a case of alkali burn treated successfully with early surgical intervention including amniotic membrane graft and forniceal reconstructionand the restored visual acuity.
CASE SUMMARY
A 23-year-old woman was referred for alkali burn of her right eye after being splashed with a drop of 40% sodium hydroxide. Slit-lamp microscopic examination showed the patient's cornea was edematous, and hazy and limbal ischemia involved half of the cornea, which can supposedly lead to eyelid deformity and symblepharon. Debridement of all necrotic tissues, immediate amniotic membrane permanent graft and transient forniceal covering with amniotic membrane were conducted a day after the burn. Corneal and conjunctival epithelial defects were completely healed in five weeks, and visual acuity was restored to 20/20 in eight weeks. Additional surgeries for allogenic limbal transplantation and autologous oral mucosal graft were performed to resolve symblepharon.
MeSH Terms
Figure
-
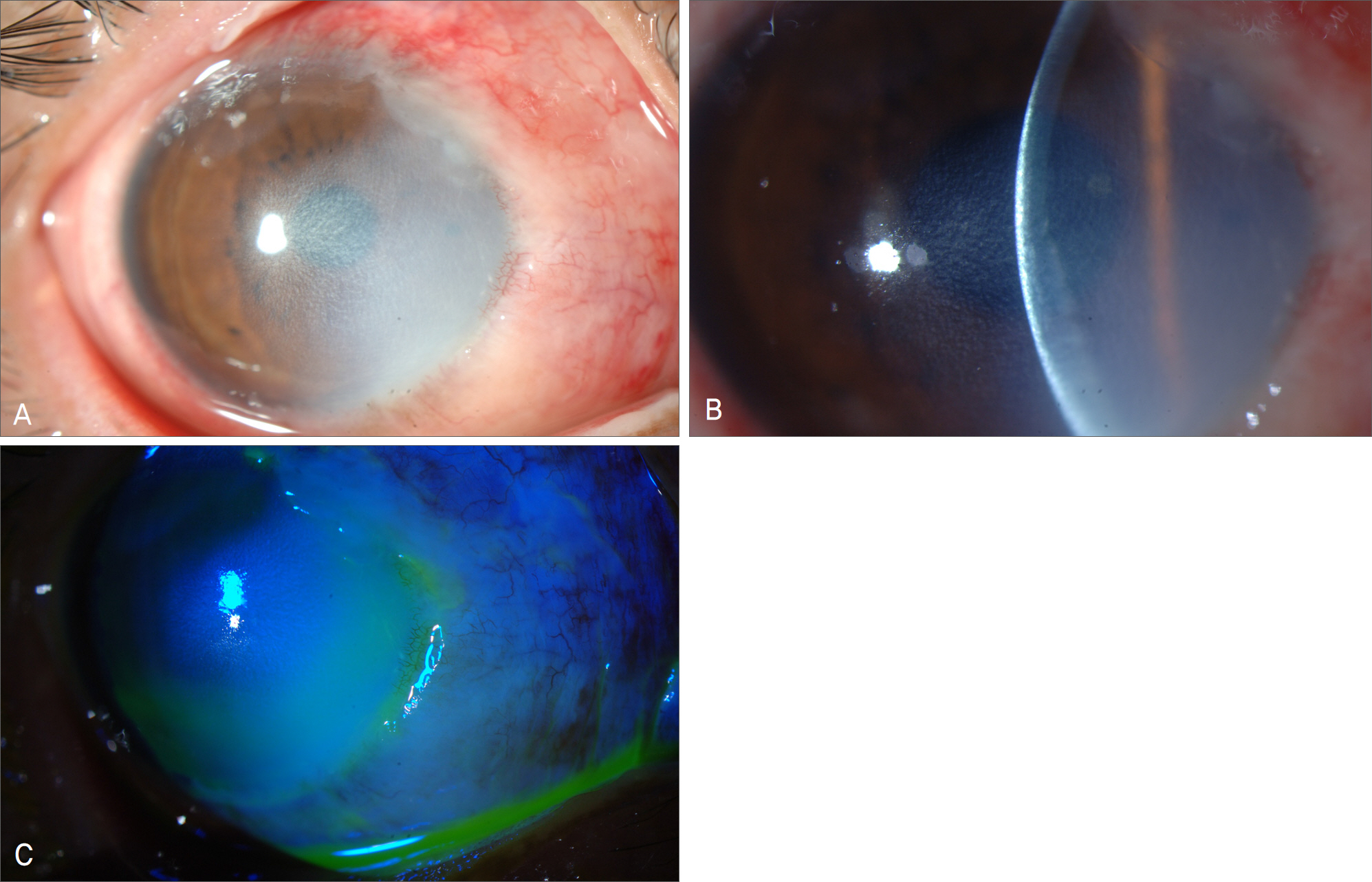
Figure 1. Slit lamp photographs. (A) Diffuse stromal edema with haziness. Note a limbal capillary ischemic change. More than half of the limbal area is ischemic. (B) Slit view shows stromal edema prominent in the inferior area. (C) Fluorescein staining reveals nearly total epithelial defect.
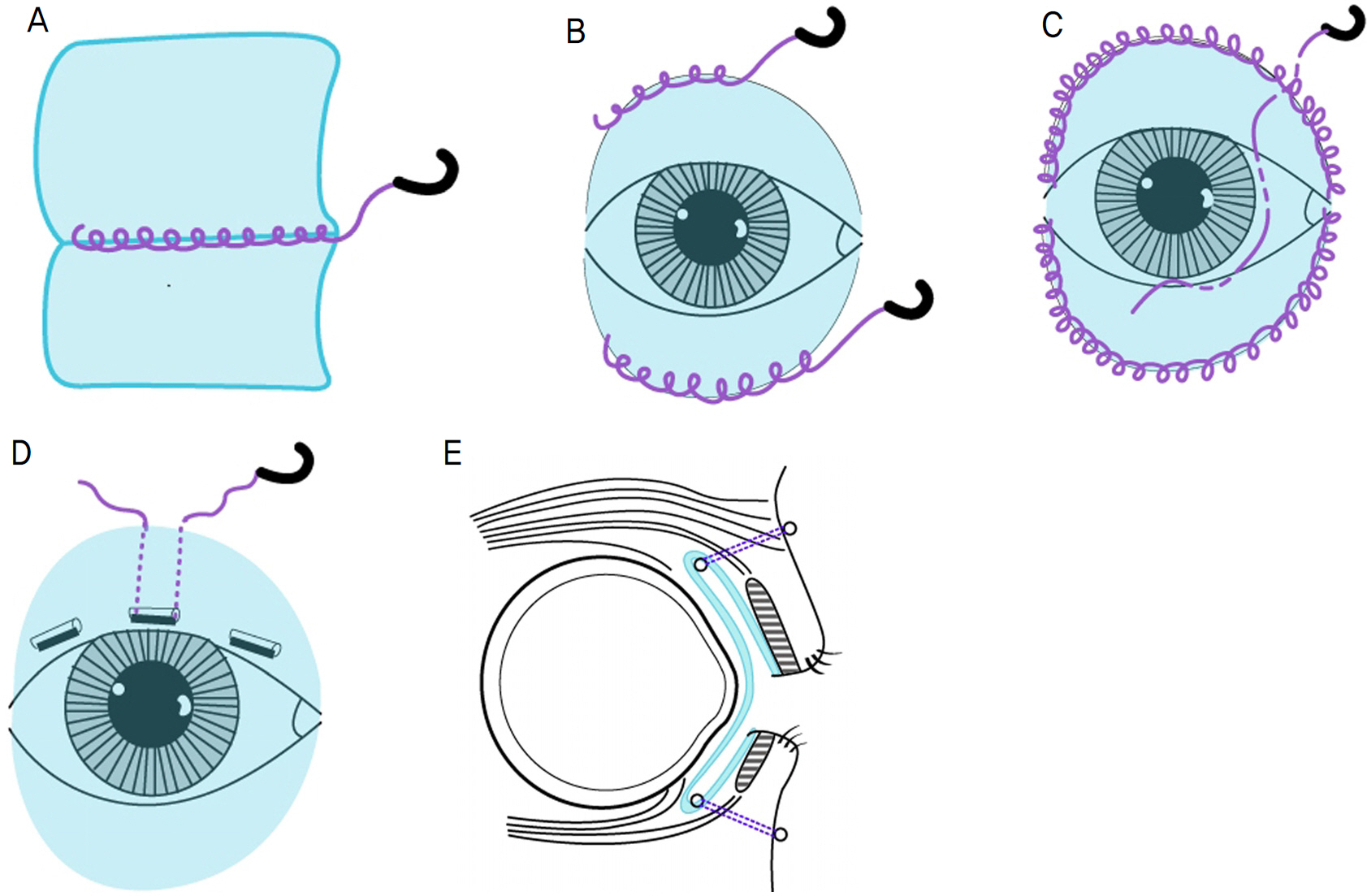
Figure 2. Schematic illustration of forniceal reconstruction with amniotic membrane graft. (A) Two amniotic membrane, 4 cm×5 cm in size, were sutured to one (4 cm×10 cm) to cover the whole bulbar and tarsal conjunctiva. (B) Sutured amniotic membrane was fixed to both eyelid margins. (C) Additional suture around the perilimbal area was done to fix redundant amniotic membrane more tight. (D) Silicone band was cut and anchored to upper and lower conjunctival fornices. (E) Sutures passed through fornices and skin bolsters, and then tied knots on each bolster.
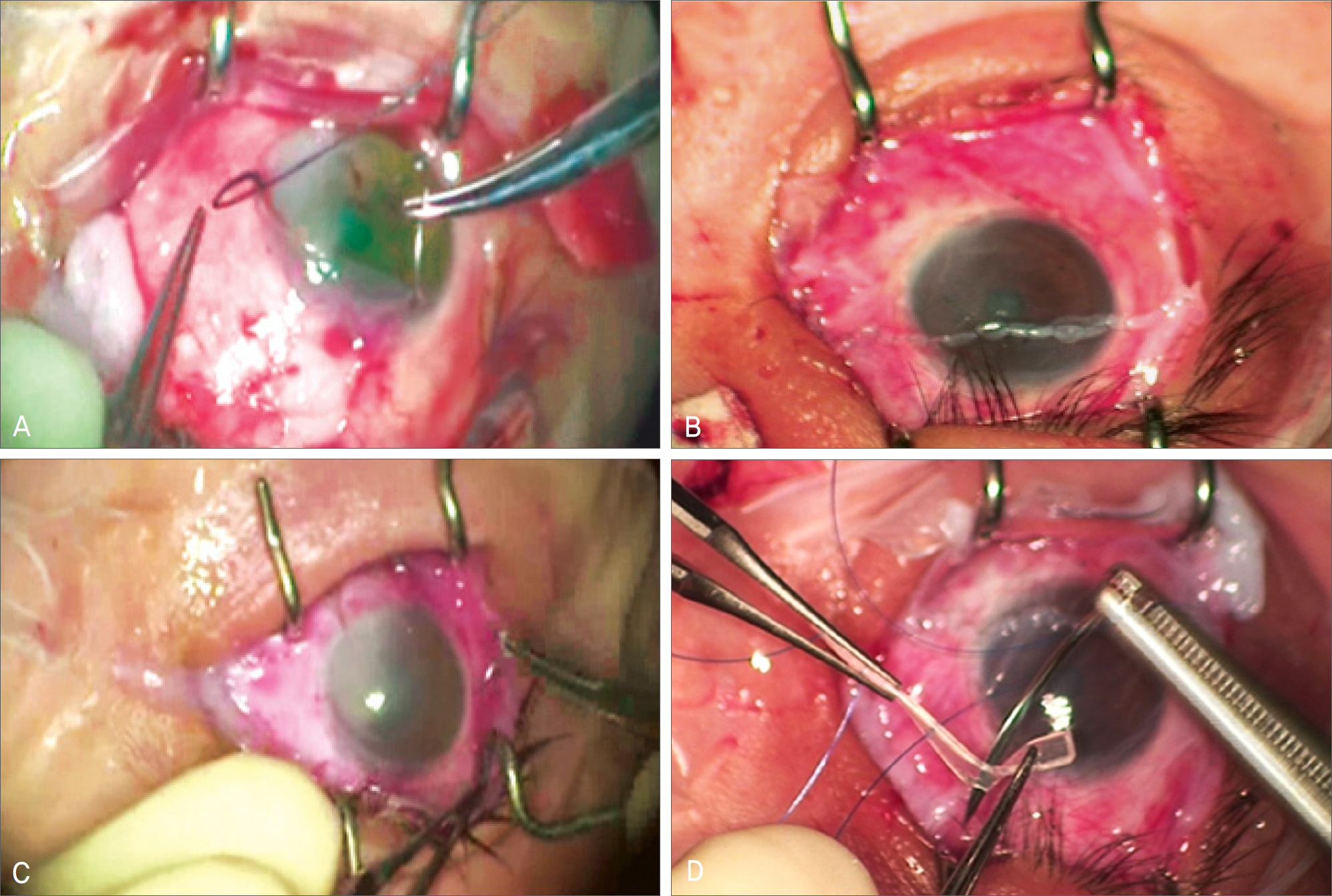
Figure 3. Photographs of operation procedure. (A) After necrotic tissue removal, permanent amniotic membrane graft is applied onto the defective area. (B) Another amniotic membrane which was doubled in size was covered over the whole cornea and bulbar and tarsal conjunctiva, thereafter it is fixed to both eyelid margins with continuous sutures. (C) Continuous suture around perilimbal area was added to fit amniotic membrane tight. (D) A silicone band is inserted to deepen both fornices over the amniotic membrane, which supports the amniotic membrane to stay tight on both inflamed tarsal and bulbar conjunctiva.
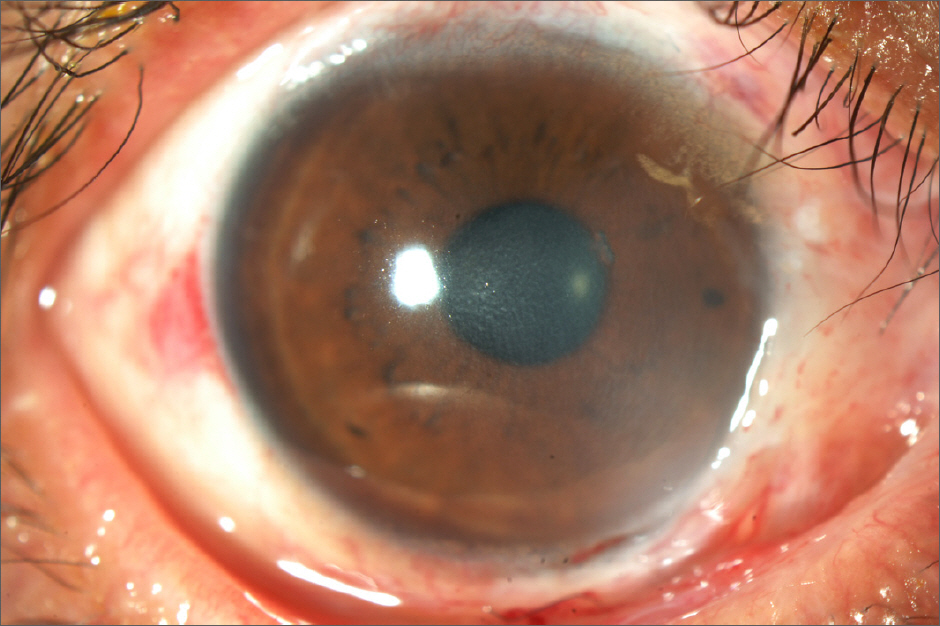
Figure 4. Follow-up photograph at 8 weeks after alkali burn. It demonstrates that corneal and conjunctival epithelial defect is completely healed and stromal opacity is markedly diminished.
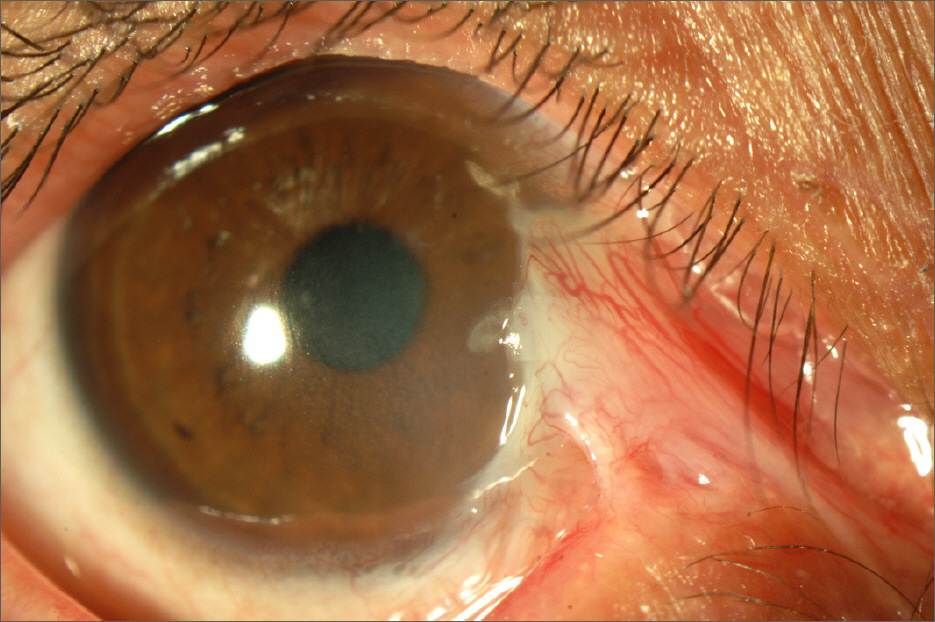
Figure 5. Follow-up photograph at 4 months after alkali burn. Note symblepharon and pseudopterygium on the nasal side of her cornea.
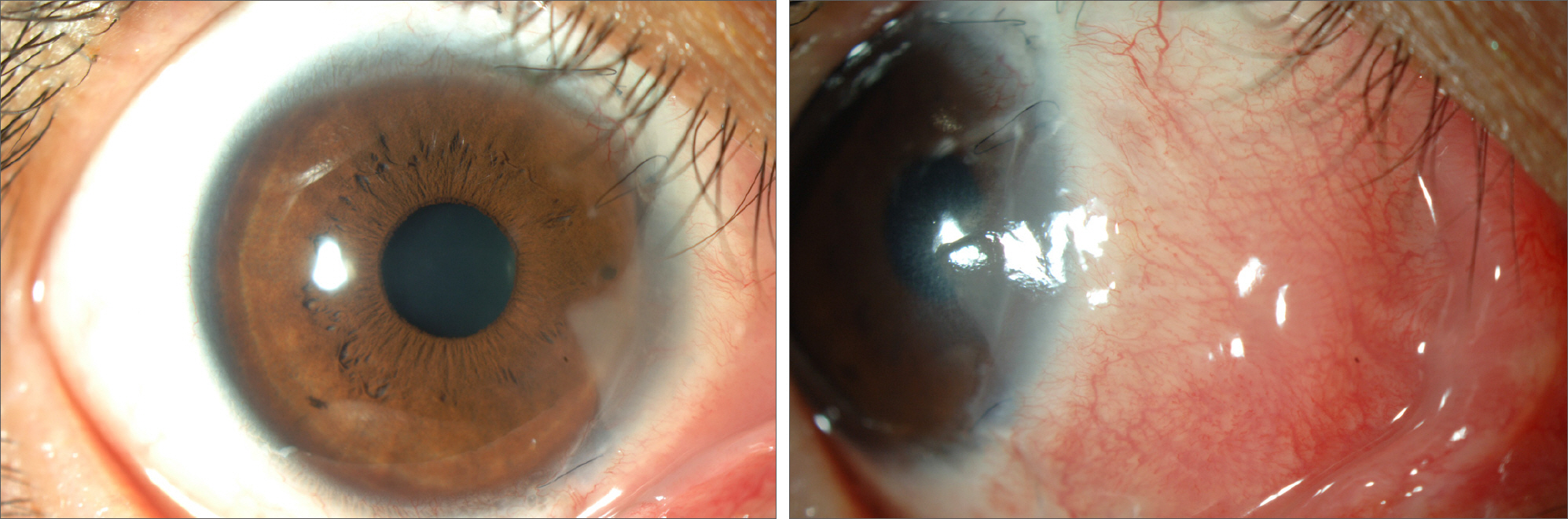
Figure 6. Photograph at 4 months after limbal transplantation, mucosal graft, and forniceal reconstruction. Symblepharon is cured and cornea is clearly maintained.
Cited by 1 articles
-
Effects of Contracted Anophthalmic Socket Reconstruction with Oral Mucosa Graft
Kyoung Hwa Bae, In Cheon You, Min Ahn
J Korean Ophthalmol Soc. 2016;57(2):188-194. doi: 10.3341/jkos.2016.57.2.188.
Reference
-
References
1. Tuft SJ, Shortt AJ. Surgical rehabilitation following severe ocular burns. Eye. 2009; 23:1966–71.
Article2. Pfister RR, Pfister DR. Alkali injuries of the eye. Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea. 2nd ed.St. Louis: Mosby;2005. v.1. chap. 103.
Article3. Roper-Hall MJ. Thermal and chemical burns. Trans Ophthalmol Soc UK. 1965; 85:631–53.4. Kheirkhah A, Johnson DA, Paranjpe DR, et al. Temporary sutureless amniotic membrane patch for acute alkaline burns. Arch Ophthalmol. 2008; 126:1059–66.
Article5. Brodovsky SC, McCarty CA, Snibson G, et al. Management of alkali burns: an 11-year retrospective review. Ophthalmology. 2000; 107:1829–35.6. Matzinger P. An innate sense of danger. Ann N Y Acad Sci. 2002; 961:341–2.
Article7. Matzinger P. The danger model: a renewed sense of self. Science. 2002; 296:301–5.
Article8. Prabhasawat P, Tesavibul N, Prakairungthong N, Booranapong W. Efficacy of amniotic membrane patching for acute chemical and thermal ocular burns. J Med Assoc Thai. 2007; 90:319–26.9. Shimmura S, Shimazaki J, Ohashi Y, Tsubota K. Antiinflammatory effects of amniotic membrane transplantation in ocular surface disorders. Cornea. 2001; 20:408–13.
Article10. Li W, He H, Kawakita T, et al. Amniotic membrane induces apop-tosis of interferon-gamma activated macrophages in vitro. Exp Eye Res. 2006; 82:282–92.11. Ko MS, Kim IS, Lee KI. A case of progressive recurrent symblepharon, treated with amniotic membrane and autograft lim-bal-conjunctiva. J Korean Ophthalmol Soc. 2000; 41:1711–6.12. Kobayashi A, Shirao Y, Yoshita T, et al. Temporary amniotic membrane patching for acute chemical burns. Eye. 2003; 17:149–58.
Article13. Wagoner MD. Chemical injuries of the eye: current concepts in pathophysiology and therapy. Surv Ophthalmol. 1997; 41:275–313.
Article14. Kim DJ, Yoon KC, Park YG. Amniotic membrane transplantation and use of adjunctive mitomycin C in the treatment of symblepharon. J Korean Ophthalmol Soc. 2005; 46:1108–13.15. Meller D, Pires RT, Mack RJ, et al. Amniotic membrane transplantation for acute chemical or thermal burns. Ophthalmology. 2000; 107:980–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Therapeutic Effect of Amniotic Membrane Extract on Keratitis Following Corneal Alkali Burn
- The Effects of Amniotic Membrane Ointment on Corneal Alkali Burn in Rabbits
- A Case of Ocular Surface Reconstruction Using Nasal and Oral Mucosa Autograft
- Amniotic Membrane Transplantation in Perforation or Impending Perforation of Cornea
- Treatment of Late Bleb Leak with Human Amniotic Membrane Transplantation
