Rifabutin Related Uveitis in AIDS: A Case Report
- Affiliations
-
- 1Department of Ophthalmology, Kyungpook National University, School of Medicine, Daegu, Korea. jpshin@hitel.net
- KMID: 2212377
- DOI: http://doi.org/10.3341/jkos.2009.50.6.951
Abstract
-
PURPOSE: To describe a case of symptomatic rifabutin-related uveitis with hypopyon and vitreous opacity in apatient with acquired immunodeficiency syndrome infected with Mycobacterium tuberculosis.
CASE SUMMARY
A 33-year-old male patient with acquired immunodeficiency syndrome was referred to our clinic for abruptly decreased vision in his right eye. Multi-drug therapy with rifabutin was administered for 5 weeks to treat tuberculosis enteritis and pulmonary tuberculosis. Visual acuity of the right eye was hand motion and hypopyon as well as vitreous opacity was found in ocular examinations. Other serologic tests, anterior chamber paracentesis and lumbar puncture test were normal. Rifabutin was immediately stopped and topical steroid and cycloplegics were administered, which resulted in resolution of the hypopyon, vitreous opacity and visual acuity. Four weeks after the initial episode, rifabutin was restarted to treat the pulmonary tuberculosis and rifabutin-related uveitis relapsed in the opposite eye.
CONCLUSIONS
Rifabutin-related uveitis should be considered in cases of uveitis in immunosuppressive patients, especially in acquired immunodeficiency syndrome patients. Underlying disease and medication history should be carefully assessed.
MeSH Terms
Figure
-
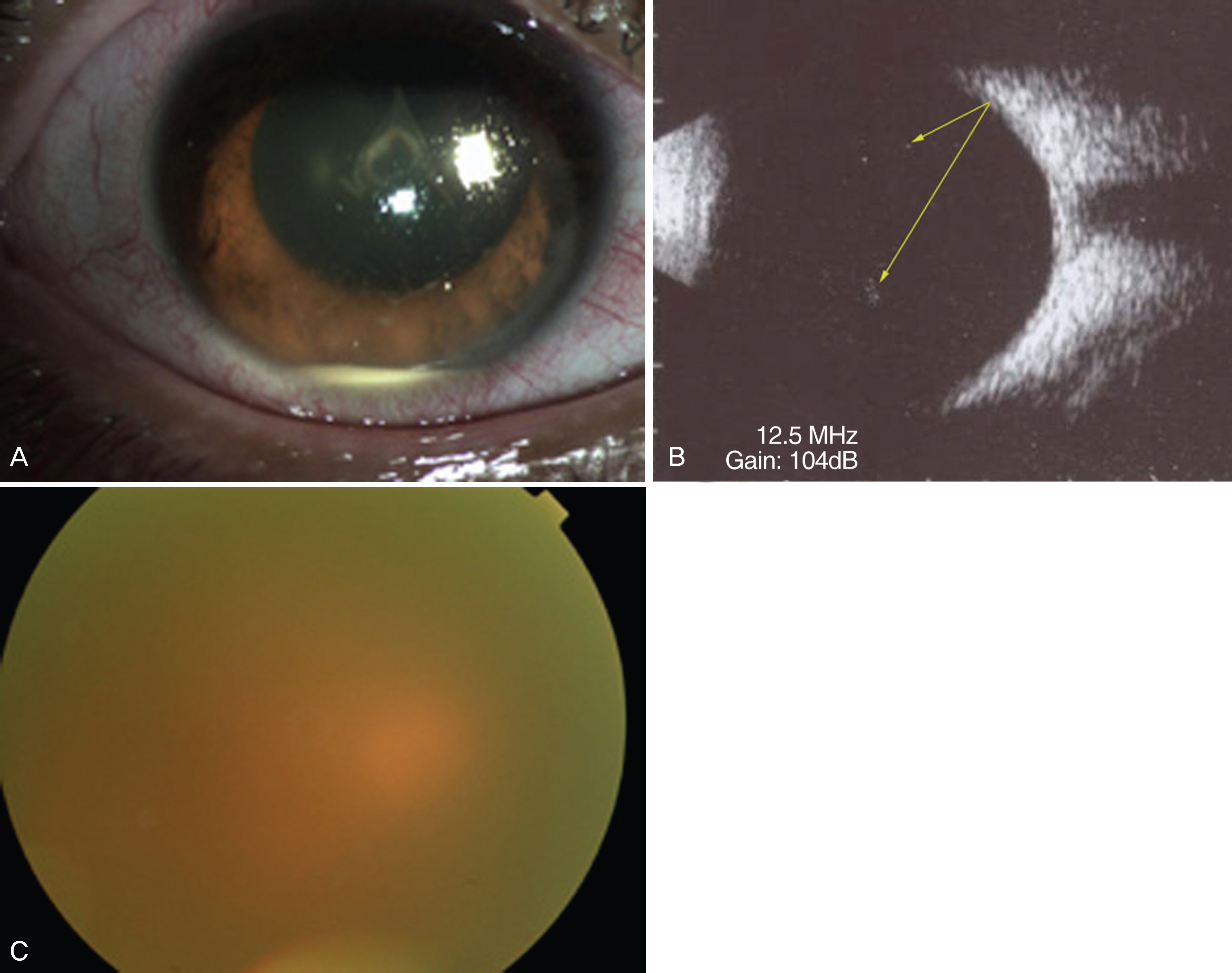
Figure 1. (A) Anterior segment photography shows hypopyon (1 mm in height) and fibrinoid reaction in the anterior chamber (AC). The grade of cells in AC was 4+. (B) The B-scan ultrasonogram shows abnormal spikes in vitreous (yellow arrows). (C) Fundus photography shows dimly seen the posterior pole due to vitreous opacity. There was no evidence of retinitis or retinal vasculitis.

Figure 2. (A) After a week of topical steroid and cycloplegic treatment, anterior chamber (AC) inflammation nearly disappeared. The grade of AC cell was trace. The lens was clear. (B) There is no evidence of retinitis or retinal vasculitis. (C) There was no evidence of macular edema and epiretinal membrane on optical coherence tomography. Visual acuity increased to 0.7.
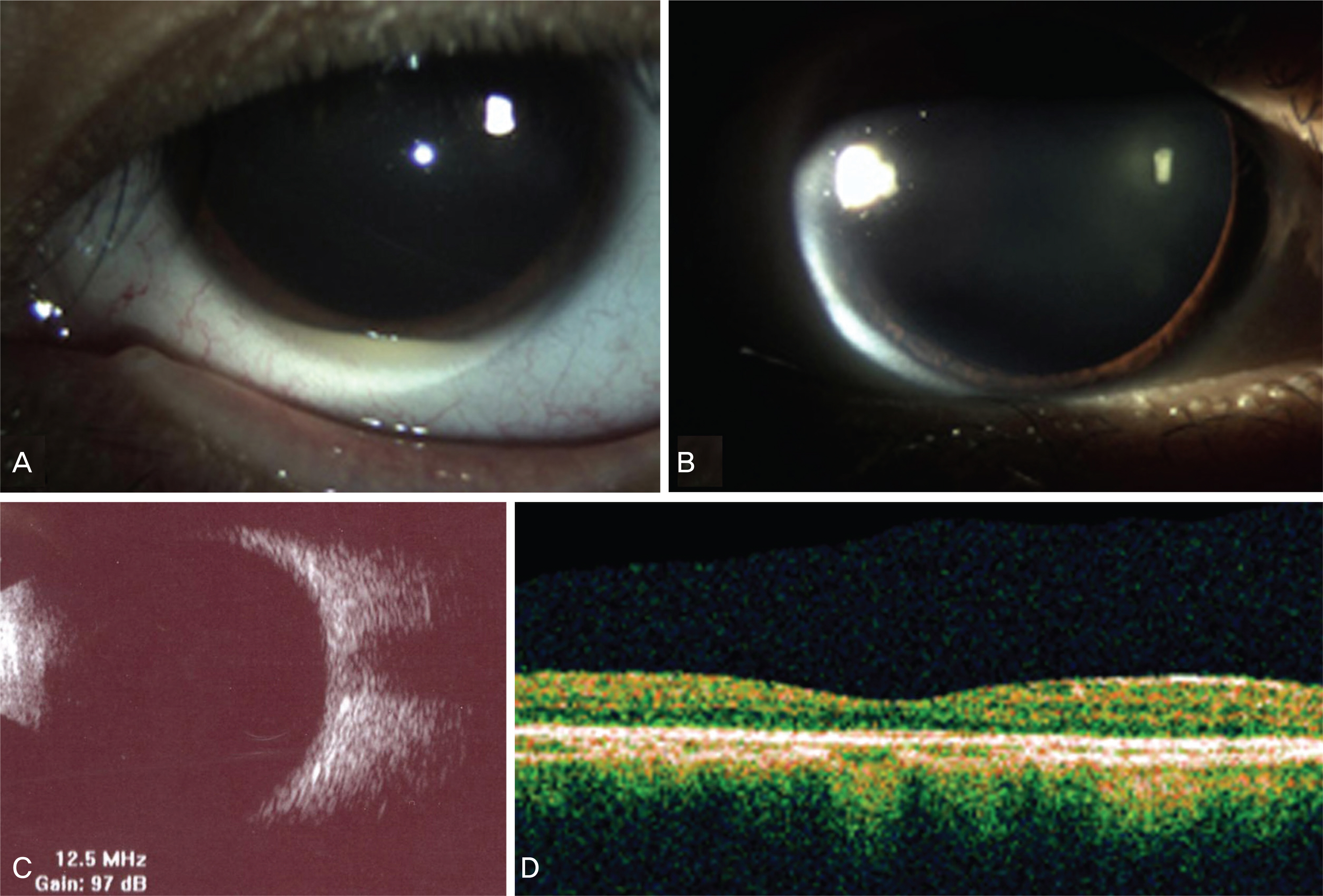
Figure 3. After 4 weeks of the initial episode, rifabutin was resumed. One month later, the patient complained of decreased visual acuity in his left eye. (A) Slit lamp examination showed hypopyon (1 mm in height) in the anterior chamber (AC) and the grade of AC cell was 4+ in the left eye. Right eye was normal. (B) Rifabutin was stopped and topical steroid and cycloplegic treatment was started in his left eye. One week after treatment, hypopyon disappeared and anterior chamber cell decreased. The grade of AC cell was 3+. (C) No retinal detachment was noted on B-scan ultrasonogram. (D) The optical coherence tomography showed no evidence of macular edema and epiretinal membrane.
Reference
-
References
1. Mandigo K, Hogg RS, Phillips P, et al. Pattern of utilization of rifabutin for prophylaxis of Mycobacterium avium complex among patients with advanced human immunodeficiency virus disease in a community setting. Tuber Lung Dis. 1996; 77:233–8.
Article2. Goble M, Iseman MD, Madsen LA, et al. Treatment of 171 patients with pulmonary tuberculosis resistant to isoniazid and rifampin. N Engl J Med. 1993; 328:527–32.
Article3. Siegal FP, Eilbott D, Burger H, et al. Dose-limiting toxicity of rifabutin in AIDS-related complex: syndrome of arthralgia/ arthritis. AIDS. 1990; 4:433–41.4. Jewelewicz DA. Schiff WM, Brown S, Barile GR. Rifabutin-associated uveitis in an immunosuppressed pediatric patient without acquired immunodeficiency syndrome. Am J Ophthalmol. 1998; 125:872–3.5. Bhagat N, Read RW, Rao N, et al. Rifabutin-associated hypopyon uveitis in human immunodeficiency virus-negative immunocompetent individual. Ophthalmology. 2001; 201:750–2.6. Shin SY, Choi J-Y, Kim YK, et al. Epidemiology of HIV/AIDS in east Asia. Infect Chemother. 2007; 39:24–37.7. Cunningham ET Jr, Margolis TP. Ocular manifestations of HIV infection. N Engl J Med. 1998; 339:236–44.
Article8. Margolis TP, Milner MS, Shama A. Herpes zoster ophthalmicus in patients with human immunodeficiency virus infection. Am J Ophthalmol. 1998; 125:285–91.
Article9. Rivero ME, Kuppermann BD, Wiley CA, et al. Acquired immunodeficiency syndrome-related intraocular B-cell lymphoma. Arch Ophthalmol. 1999; 117:616–22.
Article10. Rosberger DF, Heinemann MH, Friedberg DN, et al. Uveitis associated with human immunodeficiency virus infection. Am J Ophthalmol. 1998; 125:301–5.
Article11. Davis JL, Taskintuna I, Freeman WR, et al. Iritis and hypotony after treatment with intravenous cidofovir for cytomegalovirus retinitis. Arch Ophthalmol. 1997; 115:733–7.
Article12. Karavellas MP, Lowder CY, Macdonald C, et al. Immune recovery vitritis associated with inactive cytomegalovirus retinitis: a new syndrome. Arch Ophthalmol. 1998; 116:169–75.
Article13. Schimkat M, Althaus C, Becker K, et al. Rifabutin-associated anterior uveitis in patients infected with human immunodeficiency virus. Ger J Ophthalmol. 1996; 5:195–201.14. Moorthy RS, Valluri S, Jampol LM. Drug-induced uveitis. Surv Ophthalmol. 1998; 42:557–70.
Article15. Fuller JD, Stanfield LE, Craven DE. Rifabutin prophylaxis and uveitis. N Engl J Med. 1994; 330:1315–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Mycobacterium avium Complex Peritonitis in an Acquired Immune Deficiency Syndrome Patient
- The Proportion of Rifabutin-susceptible Strains among Rifampicin- resistant Isolates and Its Specific rpoB Mutations
- A Case of Chandler's Syndrome Associated with Anterior Uveitis
- Recurrent neutropenia induced by rifabutin in a renal transplant recipient
- The Effect of AIDS Education on Baccalaureate Nursing Students
