J Korean Surg Soc.
2010 Aug;79(2):110-115. 10.4174/jkss.2010.79.2.110.
Delta-Shaped Gastroduodenostomy after Totally Laparoscopic Distal Gastrectomy: A Comparison Analysis between Early and Late Experience
- Affiliations
-
- 1Department of Surgery, Incheon St. Mary's Hospital, The Catholic University of Korea, School of Medicine, Incheon, Korea. kjj@catholic.ac.kr
- 2Department of Surgery, Seoul St. Mary's Hospital, The Catholic University of Korea, School of Medicine, Seoul, Korea.
- KMID: 2211980
- DOI: http://doi.org/10.4174/jkss.2010.79.2.110
Abstract
- PURPOSE
We conducted this study to evaluate the feasibility and the safety of a delta-shaped gastroduodenostomy after totally laparoscopic distal gastrectomy (TLDG) and to know about the factors having influence on surgeons' performance of anastomosis and technical details of this operation.
METHODS
The clinical characteristics and the surgical results of 57 consecutive patients with delta-shaped gastroduodenostomy after TLDG at Incheon St. Mary's Hospital were reviewed. The patients were divided into 2 groups (before and after 20 cases) and their clinical characteristics and surgical results were compared. The factors which influenced the anastomotic time and the technical details of the operation were also investigated.
RESULTS
There was no difference in age, gender, body mass index, surgical results except for operation time, anastomotic time, and starting day of oral feeding between the 2 groups. The experience of the surgeon was the only factor that influenced the anastomotic time.
CONCLUSION
Delta-shaped gastroduodenostomy is a feasible and safe procedure even in the early years of a surgeon's career. It could feasibly be done in less than 20 minutes in relatively experienced hands.
MeSH Terms
Figure
-
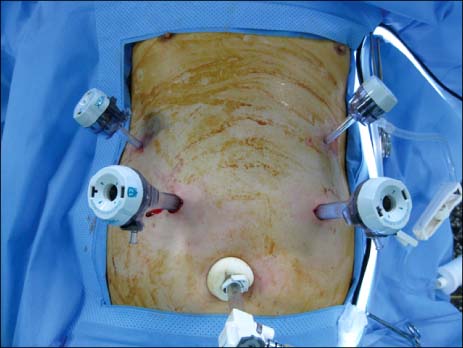
Fig. 1 Trochar placement of a delta-shaped gastroduodenostomy.

Fig. 2 Schematic illustrations for a delta-shaped gastroduodenostomy. (A) The duodenum was transected in a vertical direction rather than in the usual direction. (B) Functional end-to-end anastomosis was made between the posterior wall of the remnant stomach and the posterosuperior aspect of the duodenal bulb. (C) The entry hole for the stapler was closed by 2 consecutive staplings.
Reference
-
1. Kanaya S, Gomi T, Momoi H, Tamaki N, Isobe H, Katayama T, et al. Delta-shaped anastomosis in totally laparoscopic Billroth I gastrectomy: new technique of intraabdominal gastroduodenostomy. J Am Coll Surg. 2002. 195:284–287.2. Kim JJ, Song GY, Chin HM, Kim W, Jeon HM, Park CH, et al. The early experience with a totally laparoscopic distal gastrectomy. J Korean Gastric Cancer Assoc. 2005. 5:16–22.3. Kim JJ, Kim SK, Jun KH, Kang HC, Song KY, Chin HM, et al. Clinical usefulness of a totally laparoscopic gastrectomy. J Korean Gastric Cancer Assoc. 2007. 7:132–138.4. Lee SI, Choi YS, Park DJ, Kim HH, Yang HK, Kim MC. Comparative study of laparoscopy-assisted distal gastrectomy and open distal gastrectomy. J Am Coll Surg. 2006. 202:874–880.5. Shehzad K, Mohiuddin K, Nizami S, Sharma H, Khan IM, Memon B, et al. Current status of minimal access surgery for gastric cancer. Surg Oncol. 2007. 16:85–98.6. Song KY, Park CH, Kang HC, Kim JJ, Park SM, Jun KH, et al. Is totally laparoscopic gastrectomy less invasive than laparoscopy-assisted gastrectomy?: prospective, multicenter study. J Gastrointest Surg. 2008. 12:1015–1021.7. Kim MC, Choi HJ, Jung GJ, Kim HH. Techniques and complications of laparoscopy-assisted distal gastrectomy (LADG) for gastric cancer. Eur J Surg Oncol. 2007. 33:700–705.8. Kiyama T, Fujita I, Kanno H, Tani A, Yoshiyuki T, Kato S, et al. Laparoscopy-assisted distal gastrectomy for gastric cancer. J Gastrointest Surg. 2008. 12:1807–1811.9. Kojima K, Yamada H, Inokuchi M, Kawano T, Sugihara K. A comparison of Roux-en-Y and Billroth-I reconstruction after laparoscopy-assisted distal gastrectomy. Ann Surg. 2008. 247:962–967.10. Ryu KW, Kim YW, Lee JH, Nam BH, Kook MC, Choi IJ, et al. Surgical complications and the risk factors of laparoscopy-assisted distal gastrectomy in early gastric cancer. Ann Surg Oncol. 2008. 15:1625–1631.11. Yoo CH, Kim HO, Hwang SI, Son BH, Shin JH, Kim H. Short-term outcomes of laparoscopic-assisted distal gastrectomy for gastric cancer during a surgeon's learning curve period. Surg Endosc. 2009. 23:2250–2257.12. Bo T, Zhihong P, Peiwu Y, Feng Q, Ziqiang W, Yan S, et al. General complications following laparoscopic-assisted gastrectomy and analysis of techniques to manage them. Surg Endosc. 2009. 23:1860–1865.13. Kim JJ, Song KY, Chin HM, Kim W, Jeon HM, Park CH, et al. Totally laparoscopic gastrectomy with various types of intracorporeal anastomosis using laparoscopic linear staplers: preliminary experience. Surg Endosc. 2008. 22:436–442.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Early Experience with a Totally Laparoscopic Distal Gastrectomy
- Linear-Shaped Gastroduodenostomy in Totally Laparoscopic Distal Gastrectomy
- T-shaped Modified Delta Anastomosis as a Simple Intracorporeal Gastroduodenostomy
- Totally Laparoscopic Distal Gastrectomy after Learning Curve Completion: Comparison with Laparoscopy-Assisted Distal Gastrectomy
- Comparison of Laparoscopy-Assisted and Totally Laparoscopic Distal Gastrectomy: The Short-Term Outcome at a Low Volume Center
