J Korean Surg Soc.
2010 Mar;78(3):195-198. 10.4174/jkss.2010.78.3.195.
Paraesophageal Hernia with Small Bowel Strangulation
- Affiliations
-
- 1Department of Surgery, Chuncheon Sacred Heart Hospital, Hallym University Medical Center, Chuncheon, Korea. biogra@hallym.or.kr
- 2Department of Internal Medicine, Chuncheon Sacred Heart Hospital, Hallym University Medical Center, Chuncheon, Korea.
- KMID: 2211949
- DOI: http://doi.org/10.4174/jkss.2010.78.3.195
Abstract
- Paraesophageal hernias are usually classified into three distinct types: type I, sliding hernias; type II, paraesophageal hernias; type III, a combination of type I and II. Herniation of other abdominal organs can be classified as type IV, and is a rare situation at the esophageal hiatus. We report herein a 73-year-old female patient who presented with epigastric pain and diagnosed as type IV paraesophageal hernia. Initial evaluation was focused on myocardial ischemia. There was no evidence of myocardial ischemia in the coronary angiography, but follow-up chest X-ray revealed air-fluid levels in the left mediastinum suggested hiatal hernia. On computed tomography, herniation and strangulation of proximal jejunum into the hemithorax via left diaphragmatic defect was found. After reduction of small bowel and resection of strangulated segment, the defect was closed. Fluid collection in the hernia sac was detected at postoperative day nine, but she was discharged without complication.
Keyword
MeSH Terms
Figure
-

Fig. 1 Chest PA/lateral Jejunal dilatation in upper abdomen with air-fluid level in left mediastinum (arrow).

Fig. 2 Abdomen CT. Herniation of proximal jejunum into the hemithorax via left diaphragmatic defect. Diffuse fluid filled small bowel dilatation with suggested distal small bowel obstruction (arrow).
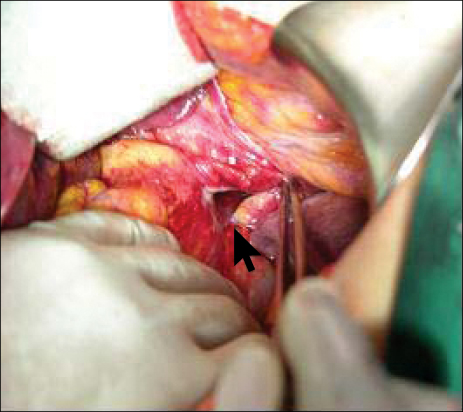
Fig. 3 Intra-operative images revealing diaphragmatic defect (arrow).
Cited by 1 articles
-
A Case of Congenital Paraesophageal Hiatal Hernia in Infancy
Won-Nyung Jang, In-Su Park, Kwi-Won Park, Seon-Young Yoo, Jin Lee, Sang-Hee Cho
Pediatr Gastroenterol Hepatol Nutr. 2012;15(2):100-104. doi: 10.5223/pghn.2012.15.2.100.
Reference
-
1. Kim HS, Baek HK. Laparoscopic repairing of diaphragmatic hernia. J Korean Surg Soc. 2005. 69:485–487.2. Kim KC, Park HJ, Yoon DS, Chi HS, Lee WJ, Lee KS, et al. A case of paraesophageal hernia repaired by laparoscopic approach. Yonsei Med J. 1996. 37:151–157.3. Itano H, Okamoto S, Kodama K, Horita N. Transthoracic Collis-Nissen repair for massive type IV paraesophageal hernia. Gen Thorac Cardiovasc Surg. 2008. 56:446–450.4. Kahrilas PJ, Kim HC, Pandolfino JE. Approaches to the diagnosis and grading of hiatal hernia. Best Pract Res Clin Gastroenterol. 2008. 22:601–616.5. Basaklar AC, Sonmez K, Karabulut R, Turkyilmaz Z, Moralioglu S. An unusual case: a giant paraesophageal hiatalhernia with intrathoracic spleen, preduodenal portal vein, malrotation, and left inferior vena cava. J Pediatr Surg. 2007. 42:e23–e25.6. Gallimidi Z, Brook OR, Militianu D, Engel A. Liver herniation through gastroesophageal hiatus of diaphragm. Eur J Radiol Extra. 2004. 51:119–120.7. Grushka JR, Grenon SM, Ferri LE. A type IV paraesophageal hernia containing a volvulized sigmoid colon. Dis Esophagus. 2008. 21:94–96.8. Sivacolundhu RK, Read RA, Marchevsky AM. Hiatal hernia controversies--a review of pathophysiology and treatment options. Aust Vet J. 2002. 80:48–53.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Laparoscopic Treatment of Paraesophageal Hernia Complicated with Gastric Volvulus
- A Case of Congenital Paraesophageal Hiatal Hernia in Infancy
- A case of paraesophageal hernia repaired by laparoscopic approach
- A Transmesenteric Hernia in a Child: Gangrene of a Long Segment of Small Bowel through a Large Mesenteric Defect
- Deceased donor liver transplantation performed one week after small bowel resection for complicated umbilical hernia: a case report
