Korean J Hepatobiliary Pancreat Surg.
2014 Aug;18(3):94-96. 10.14701/kjhbps.2014.18.3.94.
Deceased donor liver transplantation performed one week after small bowel resection for complicated umbilical hernia: a case report
- Affiliations
-
- 1Hepatobiliary-Pancreatic Center, Kyungpook National University Medical Center, Korea.
- 2Department of Surgery, Kyungpook National University School of Medicine, Daegu, Korea. mong0101@dreamwiz.com
- KMID: 1802221
- DOI: http://doi.org/10.14701/kjhbps.2014.18.3.94
Abstract
- Emergent abdominal surgery in cirrhotic patients with ascites can result in dismal postoperative outcomes such as sepsis and hepatic failure. In the present case, small bowel resection followed by anastomosis by the hand-sewn method was performed for small bowel strangulation caused by an umbilical hernia; deceased donor liver transplantation was performed one week after the bowel resection because of deterioration of hepatic function. To the best of our knowledge, this is the first case of liver transplantation performed at only one week after small bowel resection; and although we obtained a good result, the optimal time to perform liver transplantation in this situation requires further evaluation.
Figure
-
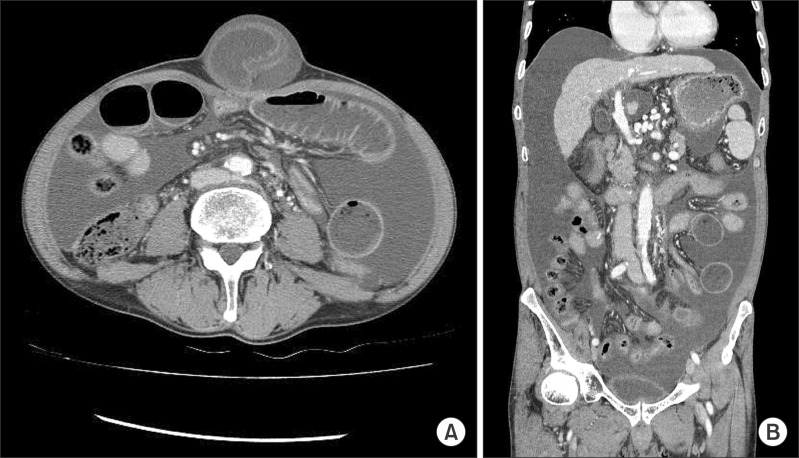
Fig. 1 Contrast-enhanced abdominal computed tomography scans of the patient showing large amount of ascites and incarcerated small bowel in the umbilical hernia. Axial view (A) and Coronal view (B).

Fig. 2 Contrast-enhanced abdominal computed tomography scans of the recipient at 1 month after deceased donor liver transplantation. A 4 cm-sized low attenuation fluid collection is present beneath the diaphragm.
Reference
-
1. Belghiti J, Durand F. Abdominal wall hernias in the setting of cirrhosis. Semin Liver Dis. 1997; 17:219–226. PMID: 9308126.
Article2. Mansour A, Watson W, Shayani V, Pickleman J. Abdominal operations in patients with cirrhosis: still a major surgical challenge. Surgery. 1997; 122:730–735. PMID: 9347849.
Article3. Telem DA, Schiano T, Divino CM. Complicated hernia presentation in patients with advanced cirrhosis and refractory ascites: management and outcome. Surgery. 2010; 148:538–543. PMID: 20346479.
Article4. Marsman HA, Heisterkamp J, Halm JA, Tilanus HW, Metselaar HJ, Kazemier G. Management in patients with liver cirrhosis and an umbilical hernia. Surgery. 2007; 142:372–375. PMID: 17723889.
Article5. Park JK, Lee SH, Yoon WJ, Lee JK, Park SC, Park BJ, et al. Evaluation of hernia repair operation in Child-Turcotte-Pugh class C cirrhosis and refractory ascites. J Gastroenterol Hepatol. 2007; 22:377–382. PMID: 17295770.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Liver retransplantation for adult recipients
- Diaphragmatic hernia following liver resection: case series and review of the literature
- Split liver transplantation for two adult recipients: A collective review of Korean experience
- Left at right heterotopic implantation of left liver graft in adult-to-adult living donor liver transplantation: the technical concern for decision-making
- A Case of Small Bowel Obstruction Due to a Paracecal Hernia
