J Korean Surg Soc.
2009 Aug;77(2):134-137. 10.4174/jkss.2009.77.2.134.
Adenoma of the Nipple
- Affiliations
-
- 1Department of Surgery, Seoul National University Bundang Hospital, Seongnam, Korea. brcakorea@gmail.com
- 2Department of Pathology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Surgery, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2211293
- DOI: http://doi.org/10.4174/jkss.2009.77.2.134
Abstract
- Adenoma of the nipple (AN) is an uncommon benign tumor of the breast. This tumor usually arises from the lactiferous ducts of the nipple. The common clinical findings are unilateral serosanguinous discharge with crust and a palpable nodule in the nipple. The symptoms and signs of AN are similar to those of Paget's disease and this confusion sometimes leads to unnecessary mastectomy. Thus performing careful clinical and histological examinations along with radiologic investigations are very important for the proper management of AN. This tumor is usually treated by total excision of the nipple. We report here on two cases of AN in two women who presented with red swelling, serosanguinous discharge and erosion of the nipple. We successfully managed them with partial excision or total excision along with reconstruction. Although AN is a relatively rare disease, surgeons should keep the diagnosis in mind for the proper management of this disease.
Figure
-
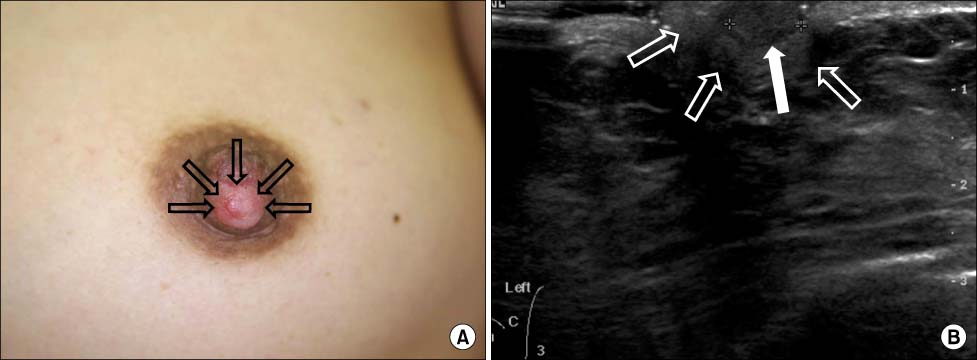
Fig. 1 (A) Preoperative appearance of the left nipple. Swelling of the left nipple with mild erythema (blank arrows) was observed. (B) Breast ultrasonographic finding. Ultrasonography shows a circumscribed oval hypoechoic mass (white arrow) in the nipple (blank arrows).
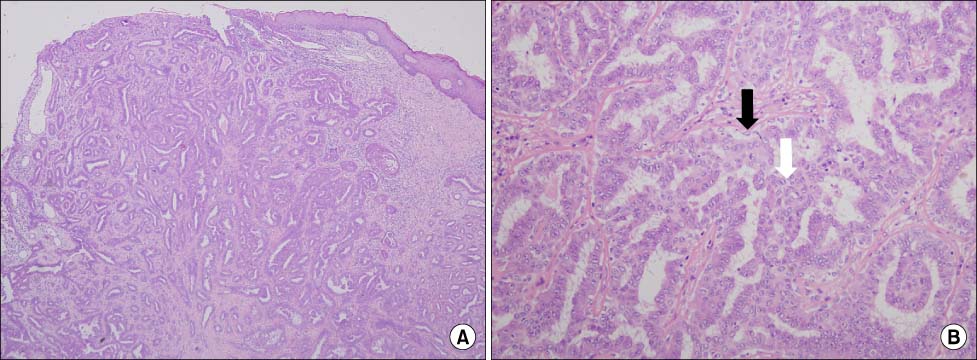
Fig. 2 (A) Low power view of the specimen. Histologic section shows a tumor in the nipple with areas of adenosis and ductal epithelial hyperplasia. Ulceration of the nipple skin is present (H&E stain, ×40). (B) Higher magnification of the specimen. Histologic section shows foci of ductal epithelial hyperplasia (white arrow) with a prominent myoepithelial layer (black arrow) (H&E stain, ×200).
Reference
-
1. Jones DB. Florid papillomatosis of the nipple ducts. Cancer. 1955. 8:315–319.2. LeGal Y, Gros CM, Bader P. L'adenomatose erosive du mamelon. Ann Anat Pathol. 1959. 4:292–304.3. Shapiro L, Karpas CM. Florid papillomatosis of the nipple. First reported case in a male. Am J Clin Pathol. 1965. 44:155–159.4. Taylor HB, Robertson AG. Adenomas of the nipple. Cancer. 1965. 18:995–1002.5. Montemarano AD, Sau P, James WD. Superficial papillary adenomatosis of the nipple: a case report and review of the literature. J Am Acad Dermatol. 1995. 33:871–875.6. Friedman EP, Hall-Craggs MA, Mumtaz H, Schneidau A. Breast MR and the appearance of the normal and abnormal nipple. Clin Radiol. 1997. 52:854–861.7. Handley RS, Thackray AC. Adenoma of nipple. Br J Cancer. 1962. 16:187–194.8. Brownstein MH, Phelps RG, Magnin PH. Papillary adenoma of the nipple: analysis of fifteen new cases. J Am Acad Dermatol. 1985. 12:707–715.9. Perzin KH, Lattes R. Papillary adenoma of the nipple (florid papillomatosis, adenoma, adenomatosis). A clinicopathologic study. Cancer. 1972. 29:996–1009.10. Lee HJ, Chung KY. Erosive adenomatosis of the nipple: Conservation of nipple by Mohs micrographic surgery. J Am Acad Dermatol. 2002. 47:578–580.
