A Case Report of Fungal Keratitis Diagnosed by Femtosecond Laser Assisted Corneal Biopsy
- Affiliations
-
- 1Department of Ophthalmology, Inje University, College of Medicine, Ilsan, Korea. jhk0924@hanmail.net
- KMID: 2211199
- DOI: http://doi.org/10.3341/jkos.2007.49.1.164
Abstract
-
PURPOSE: To describe femtosecond laser-assisted corneal biopsy and its use in assessing the causative organism in a case of fungal keratitis that occurred 8 months after penetrating keratoplasty.
CASE SUMMARY
A 27-year-old man who had undergone penetrating keratoplasty 8 months prior showed atypical diffuse corneal haze and erosion. Diagnostic corneal biopsy using a femtosecond laser was performed because of repeated negative test results for an infectious organism and a lack of improvement, despite steroid and empirical antibiotic therapy. A corneal flap 200 micrometer in depth and 3 mm in diameter was obtained. The biopsy showed pseudohyphae, which led to a diagnosis of Candidal keratitis. No complications occurred during the procedure.
CONCLUSIONS
Femtosecond laser-assisted corneal biopsy enabled identification of the infectious pathogen. This technique is easy, safe, and rapid, and it yields a biopsy specimen with a uniform depth and precise size. Femtosecond laser-assisted corneal biopsy can be used as an accurate diagnostic method in uncertain cases of corneal ulcers.
Keyword
Figure
-
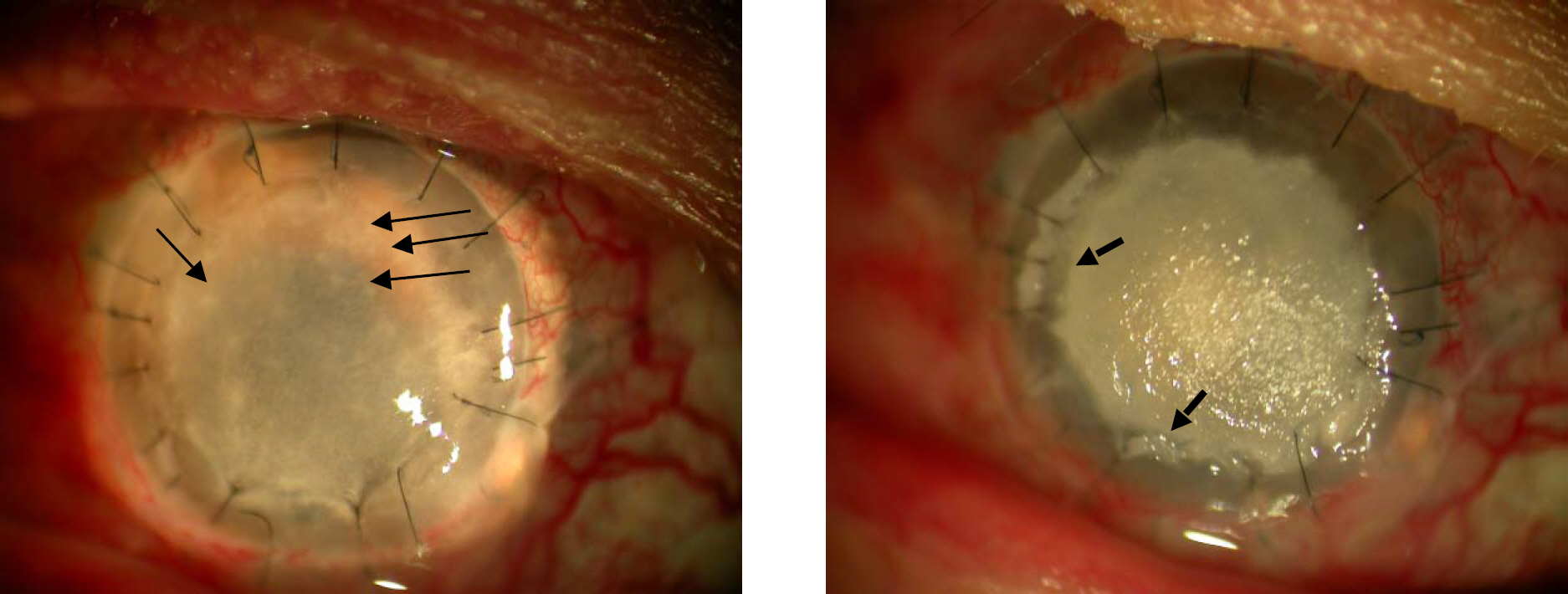
Figure 1. The photograph shows diffuse corneal haze with multiple whitish dot shape infiltrations (arrows) 8 months after keratoplasty (left). Aggravated corneal infiltration and stromal melting (dot arrows) at the margin of epithelial defect is noted 3 weeks after empirical therapy (right).

Figure 2. Center of application cone for Femtosecond laser is located at the margin of opacity by deviating eyeball toward inferotemporal side in order to get specimen containing both affected and normal tissue. Corneal biopsy (200 µm×3 mm) is being performed by Femtosecond laser (white circle).
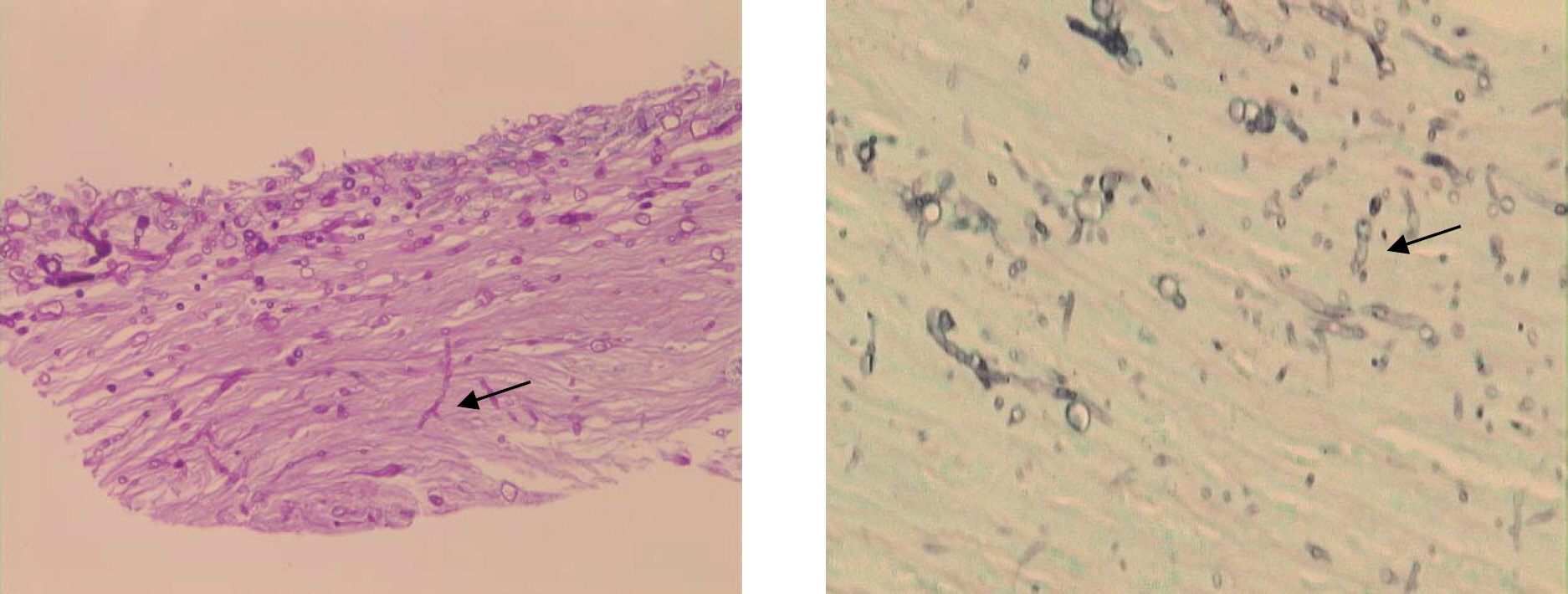
Figure 3. Spores and pseudohyphae (black arrow) invade the corneal stroma in the histopathologic examination of the biopsy tissue. (Right, periodic acid-Schiff stain, ×200; left, Gomori methenamine silver stain, ×400).
Reference
-
References
1. Alfonso EC, Rosa RH, Miller D. Fungal keratitis. Krachmer JH. Mannis MJ, Holland EJ, editors. Cornea. 2nd ed.St. Louis: Mosby;2005. 1:chap. 89.2. Kang JY, Hahn YH, Chang MW. Development of keratitis by soft contact lenses contaminated with Candidia albicans. J Korean Ophthalmol Soc. 1996; 37:945–52.3. Hahn YH, Lee DJ, Kim MS, et al. Epidemiology of fungal keratitis in Korea: A multi-center study. J Korean Ophthalmol Soc. 2000; 41:1499–508.4. Demers PE. Corneal Biopsy. Techniques in Ophthalmology. 2003; 1:92–7.
Article5. Alexandrakis G, Haimovici R, Miller D, et al. Corneal biopsy in the management of progressive microbial keratitis. Am J Ophthalmol. 2000; 129:571–6.
Article6. Newton C, Moore MB, Kaufman HE. Corneal biopsy in chronic keratitis. Arch Ophthalmol. 1987; 105:577–8.
Article7. Friedlaender MH. Corneal biopsy. Int Ophthalmol Clin. 1988; 28:101–2.
Article8. Lee P, Green WR. Corneal biopsy. Indications, techniques, and a report of a series of 87 cases. Ophthalmology. 1990; 97:718–21.9. Ishibashi Y, Kaufman HE. Corneal biopsy in the diagnosis of keratomycosis. Am J Ophthalmol. 1986; 101:288–93.
Article10. Ishibashi Y, Hommura S, Matsumoto Y. Direct examination vs culture of biopsy specimens for the diagnosis of keratomycosis. Am J Ophthalmol. 1987; 103:636–40.
Article11. Sugar A. Ultrafast (femtosecond) laser refractive surgery. Curr Opin Ophthalmol. 2002; 13:246–9.
Article12. Sarayba MA, Maguen E, Salz J, et al. Femtosecond laser keratome creation of partial thickness donor corneal buttons for lamellar keratoplasty. J Refract Surg. 2007; 23:58–65.
Article13. Terry MA, Ousley PJ, Will B. A practical femtosecond laser procedure for DLEK endothelial transplantation: cadaver eye histology and topography. Cornea. 2005; 24:453–9.14. Seitz B, Brunner H, Viestenz A, et al. Inverse mushroom- shaped nonmechanical penetrating keratoplasty using a femtosecond laser. Am J Ophthalmol. 2005; 139:941–4.15. Rabinowitz YS, Li X, Ignacio TS, Maguen E. INTACS inserts using the femtosecond laser compared to the mechanical spreader in the treatment of keratoconus. J Refract Surg. 2006; 22:764–71.
Article16. Laibson PR. Anterior Corneal Dystrophies. Krachmer JH. Mannis MJ, Holland EJ, editors. Cornea. 2nd ed.St. Louis: Mosby;2005. 1:chap. 75.
Article17. Huang AJ, Wichiensin P, Yang MC. Bacterial keratitis. Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea. 2nd ed.St. Louis: Mosby;2005. 1:chap. 81.18. Meltendorf C, Burbach GJ, Buhren J, et al. Corneal femtosecond laser keratotomy results in isolated stromal injury and favorable wound-healing response. Invest Ophthalmol Vis Sci. 2007; 48:2068–75.
Article19. Hu MY, McCulley JP, Cavanagh H, et al. Comparison of the corneal response to laser in situ keratomileusis with flap creation using the FS15 and FS30 femtosecond lasers. Clinical and confocal microscopy findings. J Cataract Refrect Surg. 2007; 33:673–81.20. Kim JY, Kim MJ, Kim TI, et al. A femtosecond laser creates a stronger flap than a mechanical microkeratome. Invest Ophthalmol Vis Sci. 2006; 47:599–604.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Excimer Laser Phototherapeutic Keratectomy for Experimental Fungal Keratitis
- Central Corneal Thickness Measured by Four Different Methods in Normal and Post-Femtosecond Laser-Assisted LASIK Eyes
- Case Report: Femtosecond Laser-Assisted Small Incision Deep Lamellar Endothelial Keratoplasty
- Early Result of Femtosecond Laser Assisted Descemet's Membrane Stripping Endothelial Keratoplasty
- Short-term Clinical Outcomes of Femtosecond Laser-assisted Cataract Surgery: Comparison with Conventional Phacoemulsification
