C1-2 Instability associated with Duplicated Vertebral Artery: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Wonkwang University, Iksan, Korea.
- 2Department of Orthopaedic Surgery, Seoul National University College of Medicine, Seoul, Korea. ortho@hananet.net
- KMID: 2209643
- DOI: http://doi.org/10.4184/jkss.2006.13.3.205
Abstract
- A vertebral artery injury is one of the most critical complications of atlantoaxial fixation. Abnormal courses or congenital anomalies of the vertebral artery increase its risk. The authors report a case of a patient who had an atlantoaxial subluxation associated with severe spinal cord compression and a duplicated vertebral artery. The atlantoaxial subluxation, which was not reduced satisfactorily by an intraoperative head position change or direct manipulation of the atlas and axis, precluded a transarticular screw fixation. The lack of free space around the spinal cord precluded a sublaminar wiring. The duplicated vertebral artery made it difficult to insert C1 lateral mass screws and C2 pedicle screws with Harms' technique.
Figure
-
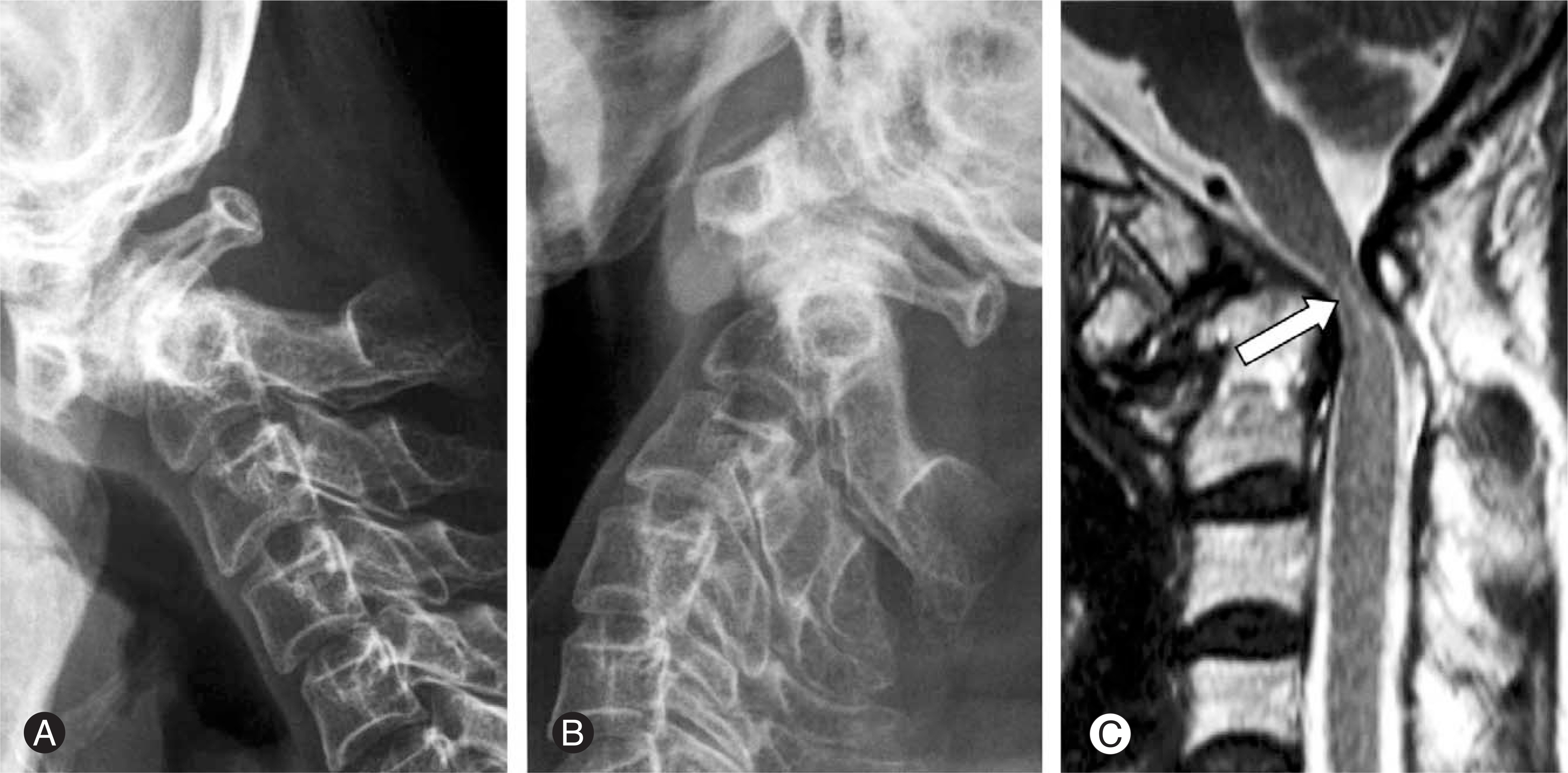
Fig. 1. Preoperative lateral radiographs of the cervical spine in flexion (A) and extension (B) show irreducible atlantoaxial subluxation and os odontoideum. A T2-weighted sagittal magnetic resonance image (C) demonstrates severe compression of the spinal cord. A high signal area in the compressed spinal cord is observed (arrow).
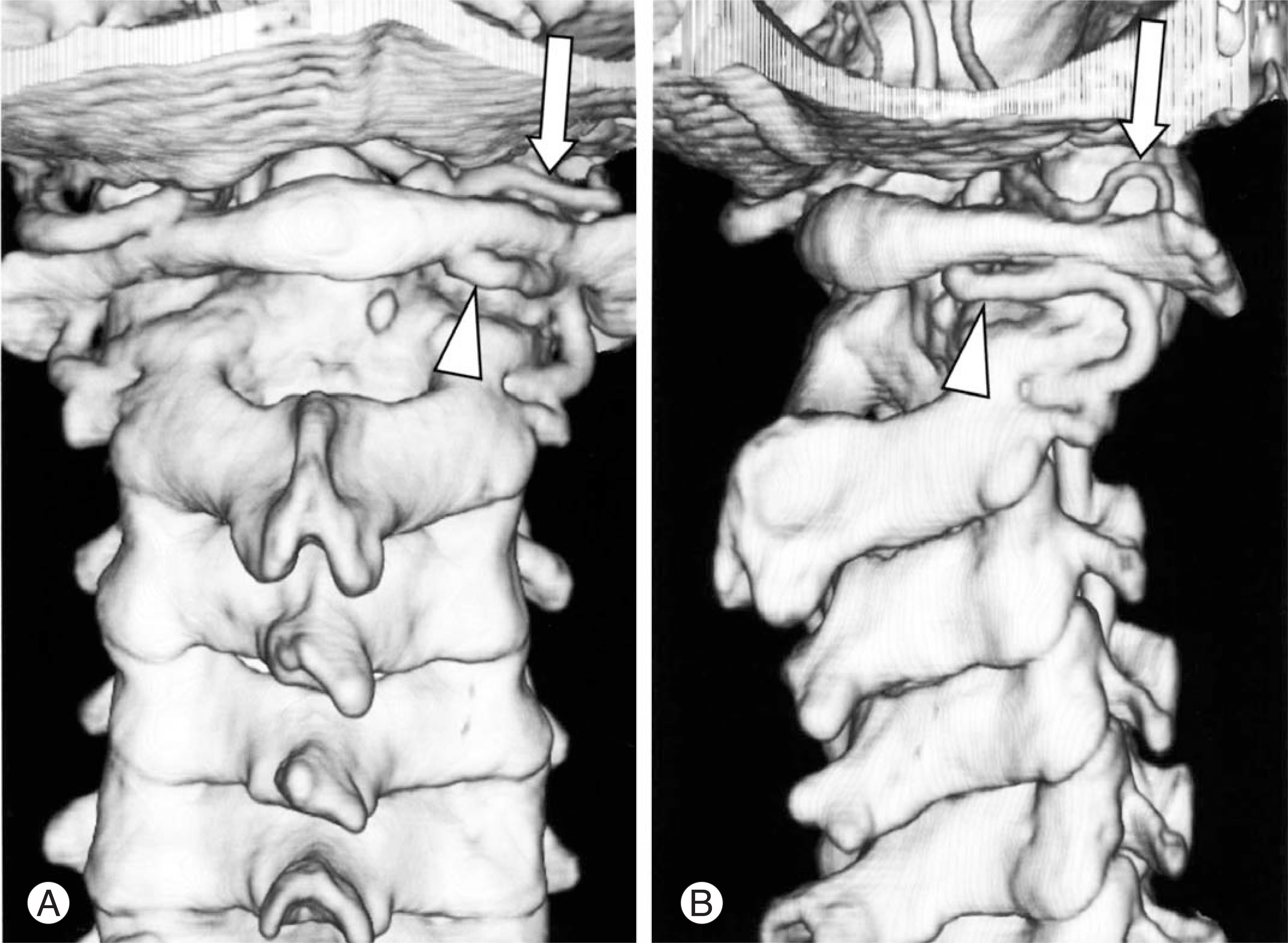
Fig. 2. CT-angiography images show duplication of the right vertebral artery. The diameter of the normal branch (arrows) is smaller than that of the aberrant branch (arrowheads).
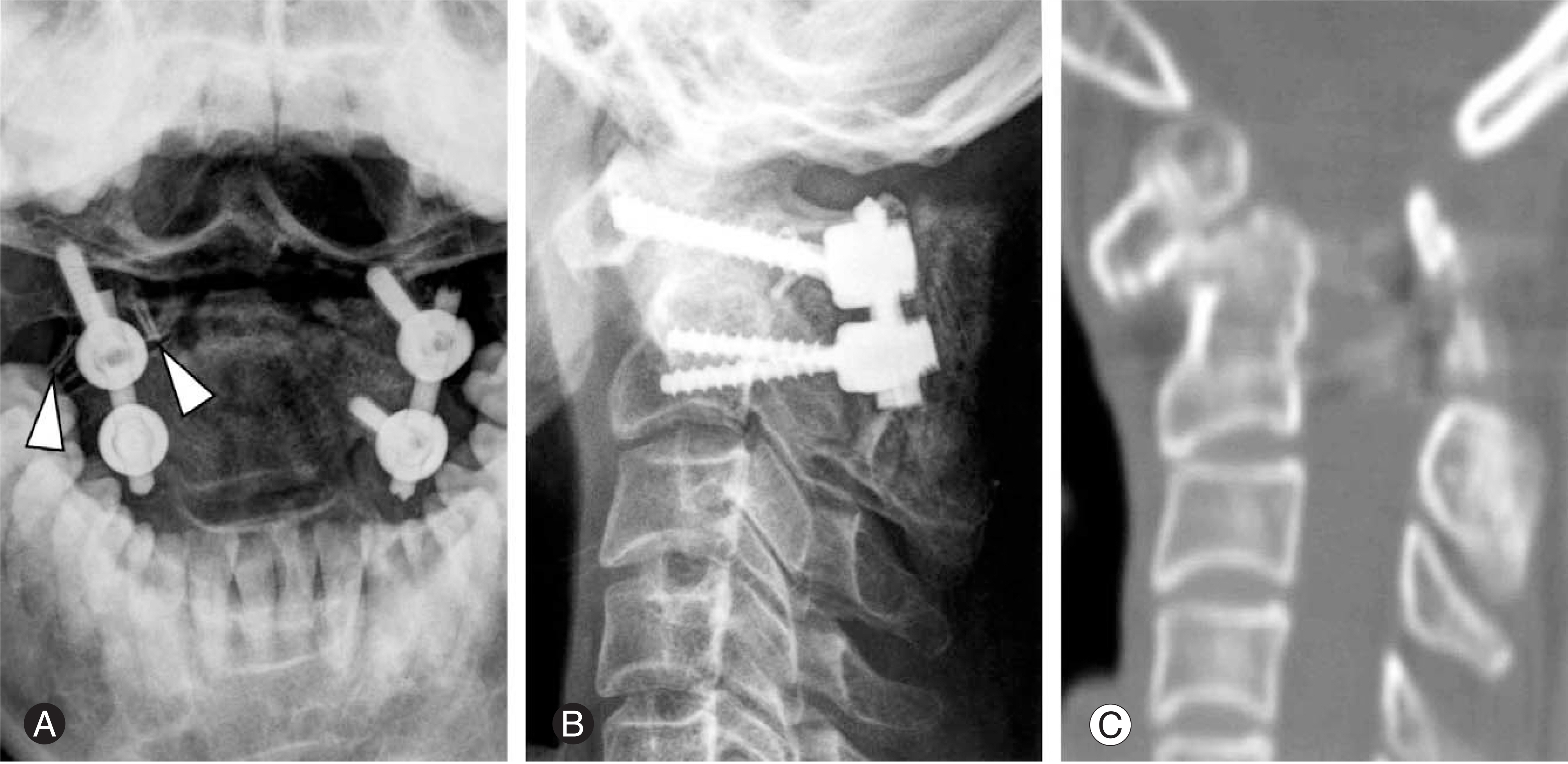
Fig. 3. Postoperative radiographs and a CT scan image are shown. On the open mouth anteroposterior view (A), vascular clips (arrowheads) used for ligation of the aberrant branch of the duplicated vertebral artery are seen on the right side. On the lateral view (B), reduction of the atlantoaxial subluxation was incomplete. However, a CT scan image (C) shows satisfactory widening of the spinal canal.
Reference
-
01). Asheesh B., Robert NH. Congenital anomalies of the cervical spine. Eismont FJ, Bell GR, editors. The Spine,. 5th ed.Philadelphia: Saunders;p. 648–652. 2006.02). Bloch O., Holly LT., Park J., Obasi C., Kim K., Johnson JP. Effect of frameless stereotaxy on the accuracy of C1-2 transarticular screw placement. J Neurosurg. 2001. 95(1 Suppl):74–79.
Article03). Harms J., Melcher RP. Posterior C1-C2 fusion with polyaxial screw and rod fixation. Spine. 2001. 26:2467–2471.
Article04). Karoly MD., Alan C. Congenital malformations of the base of the skull, atlas, and dens. Clark CR, editor. The Cervical of Spine,. 4th ed.Philadelphia: Lippincott Williams & Wilkins;p. 422–423. 2005.05). Paramore CG., Dickman CA., Sonntag VK. The anatom-ical suitability of the C1-2 complex for transarticular screw fixation. J Neurosurg. 1996. 85:221–224.
Article06). Randall TL. Congenital anomalies of the cervical spine. Frymoyer JW, Wiesel SW, editors. The Adult & Pediatric Spine,. 3rd ed.Philadelphia: Lippincott Williams & Wilkins;p. 614–615. 2004.07). Taitz C., Arensburg B. Erosion of the foramen transver-sarium of the axis. Anatomical observations. Acta Anat (Basel). 1989. 134:12–17.08). Taitz C., Nathan H., Arensburg B. Anatomical observations of the foramina transversaria. J Neurol Neurosurg Psychiatry. 1978. 41:170–176.
Article09). Tokuda K., Miyasaka K., Abe H, et al. Anomalous atlantoaxial portions of vertebral and posterior inferior cerebellar arteries. Neuroradiology. 1985. 27:410–413.
Article10). Warner WC. Anomalies of odontoid. Canale ST, editor. Campbell' s operative orthopaedics,. 10th ed.Philadelphia, Mosby;p. 1715–1733. 2003.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Duplicated Origin of the Left Vertebral Artery: A Case Report and Embryological Review
- Posterior C1-2 Stabilization Using Translaminar Screw Fixation of the Axis
- Cervicogenic Vertigo Treated by C1 Transverse Foramen Decompression : A Case Report
- Intraoperative Vertebral Artery Angiography to Guide C1-2 Transarticular Screw Fixation in a Patient with Athetoid Cerebral Palsy
- Posterior Atlantoaxial Fixation with a Combination of Pedicle Screws and a Laminar Screw in the Axis for a Unilateral High-riding Vertebral Artery
