A Case of Tracheal Adenoid Cystic Carcinoma Presenting with Diffuse Goiter
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea.
- 2Department of Otolaryngology, Chonnam National University Medical School, Gwangju, Korea.
- 3Department of Pathology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2200568
- DOI: http://doi.org/10.3803/jkes.2005.20.3.273
Abstract
- A goiter is among the most common presenting symptoms of patients with thyroid diseases and is usually caused by intrinsic thyroid problems. While direct invasion of the trachea by aggressive thyroid tumors is a well-known phenomenon, the reverse situation, that is, a primary tracheal neoplasm invading by direct extension into the thyroid gland, presenting with a goiter is very rare. Here, a case of a tracheal adenoid cystic carcinoma(ACC), presenting with a diffuse goiter, is reported. A 47-year-old woman presented with slowly growing anterior neck swelling. A physical examination showed a diffuse firm goiter. The patient was euthyroiditic, and serum negative for thyroid autoantibodies. Thyroid ultrasonography and neck CT revealed a doughnut-shaped mass, encircling the trachea and displacing the thyroid anteriorly. Ultrasonography-guided fine needle aspiration(FNA) was compatible with an ACC, and a subsequent surgical resection confirmed the diagnosis. Although the occurrence of a tracheal ACC invading the thyroid is rare, this case highlights the need to be aware of unusual lesions arising in the region of the thyroid. This knowledge will help in making the correct cytological diagnosis when these lesions are sampled by FNA
MeSH Terms
Figure
-
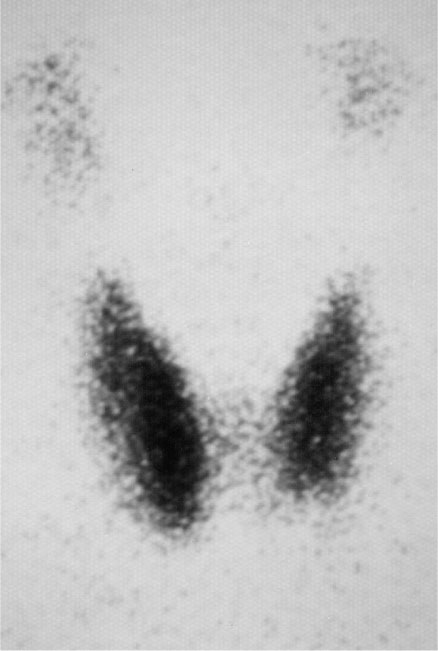
Fig. 1 99m-Technetium thyroid scan taken 3 years ago shows normal thyroid gland

Fig. 2 Mild diffuse goiter is evident in anterior portion of the neck
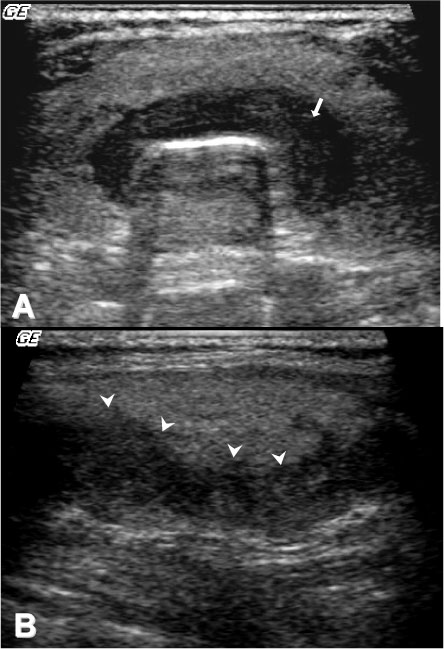
Fig. 3 Thyroid ultrasonograms. A transverse scan over the isthmus shows a well-defined horseshoe-shaped hypoechoic mass (arrow in panel A). A longitudinal scan shows the extent of the lesion (panel B). Some lobular portions are observed along the tumor margin (arrowheads in panel B)
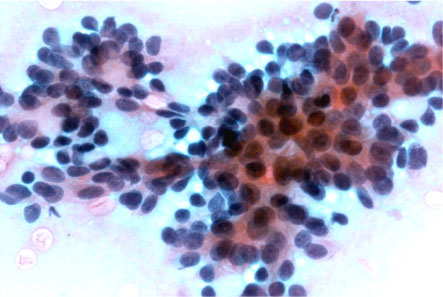
Fig. 4 Fine-needle aspiration cytology shows classic hyaline globules and tight clusters of basaloid cells (Pap, ×400)
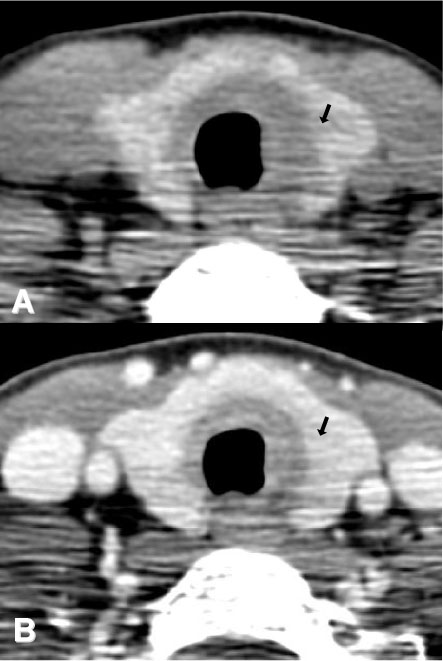
Fig. 5 A doughnut-shaped low density lesion encircling the trachea contrasts well with the iodine-rich thyroid gland in a pre-contrast neck CT scan (arrow in panel A). A post-contrast neck CT scan well delineates the mass (arrow in panel B)
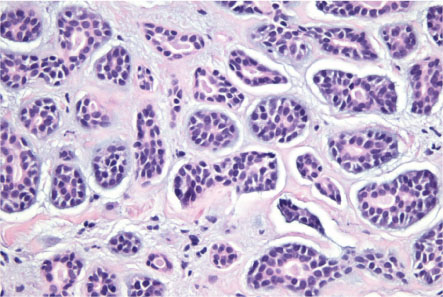
Fig. 6 Histology confirms the diagnosis of adenoid cystic carcinoma. The tumor cells have a bland, uniform appearance. Tubular structures with bicellular layers are also noted (H & E, ×200)
Reference
-
1. Hennessey JV. Braverman , Utiger Robert D, editors. Physical examination of the thyroid gland. The thyroid. A fundamental and clinical text. 2004. 9th ed. Philadelphia: Lippincott Williams & Wilkins Co;392–397.2. Bradley PJ. Adenoid cystic carcinoma of the head and neck: a review. Curr Opin Otolaryngol Head Neck Surg. 2004. 12:127–132.3. Zirkin HJ, Tovi F. Tracheal carcinoma presenting as a thyroid tumor. J Surg Oncol. 1984. 26:268–271.4. Mahnke CG, Werner JA, Lippert BM, Schluter E, Rudert H. Adenoid cystic carcinoma of the trachea. Case report and review of the literature on malignant tracheal tumors. Laryngorhinootologie. 1994. 73:445–448.5. Na DG, Han MH, Kim KH, Chang KH, Yeon KM. Primary adenoid cystic carcinoma of the cervical trachea mimicking thyroid tumor: CT evaluation. J Comput Assist Tomogr. 1995. 19:559–563.6. Tsue TT, Wood DE, True LD, Weymuller EA Jr. Male presenting with hoarseness and a thyroid mass. Am J Otolaryngo. 1995. 16:158–164.7. Natarajan S, Greaves TS, Raza AS, Cobb CJ. Fine-needle aspiration of an adenoid cystic carcinoma of the larynx mimicking a thyroid mass. Diagn Cytopathol. 2004. 30:115–118.8. Idowu MO, Reiter ER, Powers CN. Adenoid cystic carcinoma: a pitfall in aspiration cytology of the thyroid. Am J Clin Patho. 2004. 121:551–556.9. Haji BE, Ahmed MS, Prasad A, Omar MS, Das DK. Papillary thyroid carcinoma with an adenoid cystic pattern: report of a case with fine-needle aspiration cytology and immunocytochemistry. Diagn Cytopathol. 2004. 30:418–421.10. Yamazaki K. Unique follicular carcinoma of the thyroid gland with extracellular deposition of amorphous globular structures mimicking an adenoid cystic pattern. Virchows Arch. 2003. 443:690–692.15. Kwak SH, Lee KS, Chung MJ, Jeong YJ, Kim GY, Kwon OJ. Adenoid cystic carcinoma of the airways: helical CT and histopathologic correlation. Am J Roentgenol. 2004. 183:277–281.
