J Korean Neurotraumatol Soc.
2010 Jun;6(1):38-42. 10.13004/jknts.2010.6.1.38.
Analysis of the Computed Tomographic Findings Related with the Mean Duration of Brain Expansion after the Operation of Chronic Subdural Hematoma
- Affiliations
-
- 1Department of Neurosurgery, Seoul Veterans Hospital, Seoul, Korea. colloseum@freechal.com
- KMID: 2192361
- DOI: http://doi.org/10.13004/jknts.2010.6.1.38
Abstract
OBJECTIVE
The purpose of this study is evaluate the radiological factors related with the mean duration of brain expansion for after chronic subdural hematoma surgery.
METHODS
From January 2007 to June 2009, 44 patients were taken operation for chronic subdural hematoma using burr hole on our hospital. Among them, seven patients were excluded. One was taken craniotomy after burr hole drainage due to subdural abscess and the remaining six patients whose brains failed to show complete expansion postoperatively in at least three months of follow-up. We retrospectively analyzed the mean duration of brain expansion by following five aspects: the maximal thickness of preoperative hematoma, degree of midline shift, density of preoperative hematoma, presence or absence of contralateral side hematoma, and degree of postoperative pneumocephalus.
RESULTS
When preoperative or postoperative computed tomographic images were put into analysis, the radiologic factors such as preoperative hematoma with the maximal thickness more than 20 mm, midline shifting more than 10 mm, hematoma of mixed density, presence of contralateral side hematoma, postoperative large air collection had taken more time for their brains to expand. Four out of six patients with contralateral side hematoma whose maximal thickness were more than 10 mm on the preoperative computed tomographic images have needed additional surgery on the contralateral side after initial burr hole trephination with hematoma drainage.
CONCLUSION
Among the factors been analyzed for brain expansion in this study, the presence of contralateral side hematoma and postoperative large pneumocephalus were proven to be statistically significant radiologic factors for delaying the expansion of the brains. Thus, the efforts to reduce postoperative air collection should be made as surgeons' aspect. In addition, bilateral surgery simultaneously should also be recommended, especially when the maximal thickness of contralateral hematoma is more than 10 mm, even though this specific thickness of hematoma was not tested statistically.
Keyword
MeSH Terms
Figure
-
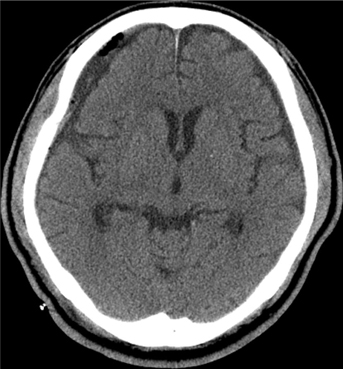
FIGURE 1 Postoperative CT scan showing slit-like pneumocephalus.
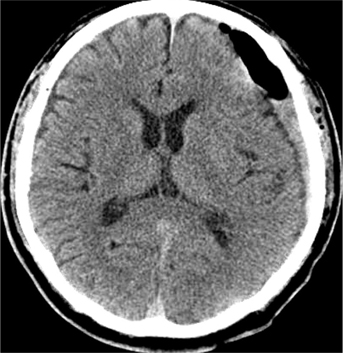
FIGURE 2 Postoperative CT scan showing large pneumocephalus.
Reference
-
1. Ernestus RI, Beldzinski P, Lanfermann H, Klug N. Chronic subdural hematoma: surgical treatment and outcome in 104 patients. Surg Neurol. 1997; 48:220–225.
Article2. Erol FS, Topsakai C, Faik Ozveren M, Kaplan M, Tiftikci MT. Irrigation vs. closed drainage in the treatment of chronic subdural hematoma. J Clin Neurosci. 2005; 12:261–263.
Article3. Gelabert-González M, Iglesias-Pais M, García-Allut A, Martínez-Rumbo R. Chronic subdural haematoma: surgical treatment and outcome in 1,000 cases. Clin Neurol Neurosurg. 2005; 107:223–229.
Article4. Han HJ, Park CW, Kim EY, Yoo CJ, Kim YB, Kim WK. One vs. two burr hole craniostomy in surgical treatment of chronic subdural hematoma. J Korean Neurosurg Soc. 2009; 46:87–92.
Article5. Kim JH, Kwon TH, Han S, Kim JH, Park YK, Chung HS. Clinical evaluation of bilateral chronic subdural hematoma: characteristic findings and significance of postoperative drainage amount. J Korean Neurotraumatol Soc. 2005; 1:46–50.
Article6. Ko BS, Lee JK, Seo BR, Moon SJ, Kim JH, Kim SH. Clinical analysis of risk factors related to recurrent chronic subdural hematoma. J Korean Neurosurg Soc. 2008; 43:11–15.
Article7. Lee JK, Choi JH, Kim CH, Lee HK, Moon JG. Chronic subdural hematomas a comparative study of three types of operative procedures. J Korean Neurosurg Soc. 2009; 46:210–214.8. Markwalder TM. The course of chronic subdural hematomas after burr-hole craniostomy with and without closed-system drainage. Neurosurg Clin N Am. 2000; 11:541–546.
Article9. Markwalder TM, Steinsiepe KF, Rohner M, Reichenbach W, Markwalder H. The course of chronic subdural hematomas after burr-hole craniostomy and closed-system drainage. J Neurosurg. 1981; 55:390–396.
Article10. Mondorf Y, Abu-Owaimer M, Gaab MR, Oertel JM. Chronic subdural hematoma--craniotomy versus burr hole trephination. Br J Neurosurg. 2009; 23:612–616.11. Mori K, Maeda M. Surgical treatment of chronic subdural hematoma in 500 consecutive cases: clinical characteristics, surgical outcome, complications, and recurrence rate. Neurol Med Chir (Tokyo). 2001; 41:371–381.
Article12. Okada Y, Akai T, Okamoto K, Iida T, Takata H, Iizuka H. A comparative study of the treatment of chronic subdural hematoma--burr hole drainage versus burr hole irrigation. Surg Neurol. 2002; 57:405–409. discussion 410.
Article13. Santarius T, Kirkpatrick PJ, Ganesan D, Chia HL, Jalloh I, Smielewiski P, et al. Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: a randomised controlled trial. Lancet. 2009; 374:1067–1073.
Article14. Stanisic M, Lund-Johansen M, Mahesparan R. Treatment of chronic subdural hematoma by burr-hole craniostomy in adults: influence of some factors on postoperative recurrence. Acta Neurochir (Wien). 2005; 147:1249–1256. discussion 1256-1257.
Article15. Suzuki K, Sugita K, Akai T, Takahata T, Sonobe M, Takahashi S. Treatment of chronic subdural hematoma by closed-system drainage without irrigation. Surg Neurol. 1998; 50:231–234.
Article16. Torihashi K, Sadamasa N, Yoshida K, Narumi O, Chin M, Yamagata S. Independent predictors for recurrence of chronic subdural hematoma a review of 343 consecutive surgical cases. Neurosurgery. 2008; 63:1125–1129. discussion 1129.17. Tsai TH, Lien AS, Hwang SL, Hwang TY, Hwang YF. A comparative study of the patients with bilateral or unilateral chronic subdural hematoma precipitating factors and postoperative outcomes. J Trauma. 2010; 68:571–575.
Article18. Wakai S, Hashimoto K, Watanabe N, Inoh S, Ochiai C, Nagai M. Efficacy of closed-system drainage in treating chronic subdural hematoma: a prospective comparative study. Neurosurgery. 1990; 26:771–773.
Article19. Yu GJ, Han CZ, Zhang M, Zhuang HT, Jiang YG. Prolonged drainage reduces the recurrence of chronic subdural hematoma. Br J Neurosurg. 2009; 23:606–611.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship of Fibrinogen Degradation Products to Clinical Findings in Chronic Subdural Hematoma
- Factors Affecting Brain Re-expansion after Simple Burr Hole Drainage in Chronic Subdural Hematoma
- Evolution of Chronic Subdural Hematoma based on Brain CT findings and Appropriate Treatment Methods
- Clinical Analysis of Chronic Subdural Hematoma
- Factors Affecting the Reaccumulation of Chronic Subdural Hematoma after Burr-hole Trephination and Closed-system Drainage
