The Risk Factors for Hydrocephalus and Subdural Hygroma after Decompressive Craniectomy in Head Injured Patients
- Affiliations
-
- 1Department of Neurosurgery, Daejeon St. Mary's Hospital, The Catholic University of Korea College of Medicine, Daejeon, Korea. hyungjin@catholic.ac.kr
- KMID: 2191378
- DOI: http://doi.org/10.3340/jkns.2015.58.3.254
Abstract
OBJECTIVE
The present study aims to investigate 1) the risk factors for hydrocephalus and subdural hygroma (SDG) occurring after decompressive craniectomy (DC), and 2) the association between the type of SDG and hydrocephalus.
METHODS
We retrospectively reviewed the clinical and radiological features of 92 patients who underwent DC procedures after severe head injuries. The risk factors for developing post-traumatic hydrocephalus (PTH) and SDG were analyzed. Types of SDGs were classified according to location and their relationship with hydrocephalus was investigated.
RESULTS
Ultimately, 26.09% (24/92) of these patients developed PTH. In the univariate analyses, hydrocephalus was statically associated with large bone flap diameter, large craniectomy area, bilateral craniectomy, intraventricular hemorrhage, contralateral or interhemisheric SDGs, and delayed cranioplasty. However, in the multivariate analysis, only large craniectomy area (adjusted OR=4.66; p=0.0239) and contralateral SDG (adjusted OR=6.62; p=0.0105) were significant independent risk factors for developing hydrocephalus after DC. The incidence of overall SDGs after DC was 55.43% (51/92). Subgroup analysis results were separated by SDG types. Statistically significant associations between hydrocephalus were found in multivariate analysis in the contralateral (adjusted OR=5.58; p=0.0074) and interhemispheric (adjusted OR=17.63; p=0.0113) types.
CONCLUSION
For patients who are subjected to DC following severe head trauma, hydrocephalus is associated with a large craniectomy area and contralateral SDG. For SDGs after DC that occur on the interhemispherical or controlateral side of the craniectomy, careful follow-up monitoring for the potential progression into hydrocephalus is needed.
MeSH Terms
Figure
-
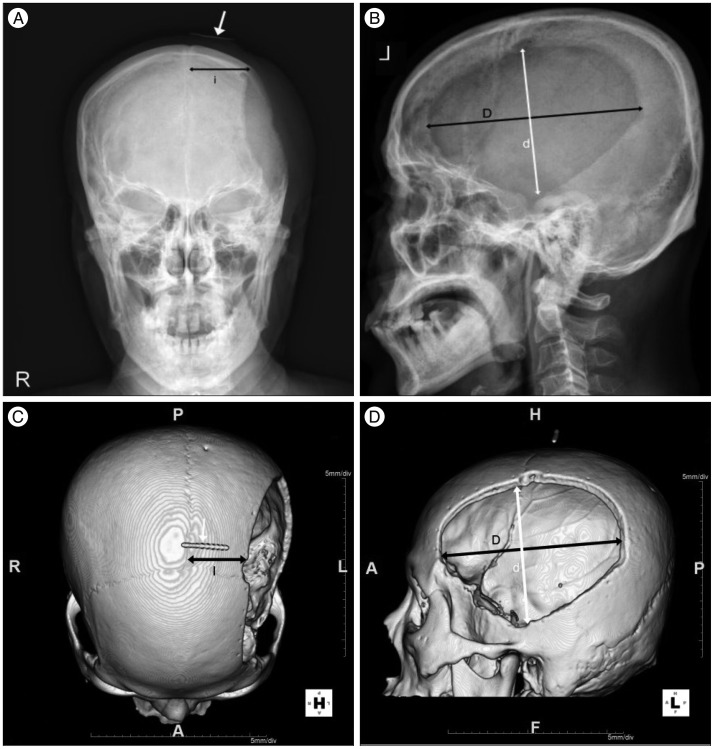
Fig. 1 Skull AP (A), lateral (B), and 3D CT reconstruction (C : from above, D : from lateral) with real 3 cm marker after decompressive craniectomy. Distance from midline of skull AP (i) is 123% larger than the true distance on the 3D CT (I), as shown through a compared with a real 3 cm marker (white arrow). Largest AP diameter (D), distance perpendicular to D (d). AP : antero-posterior.
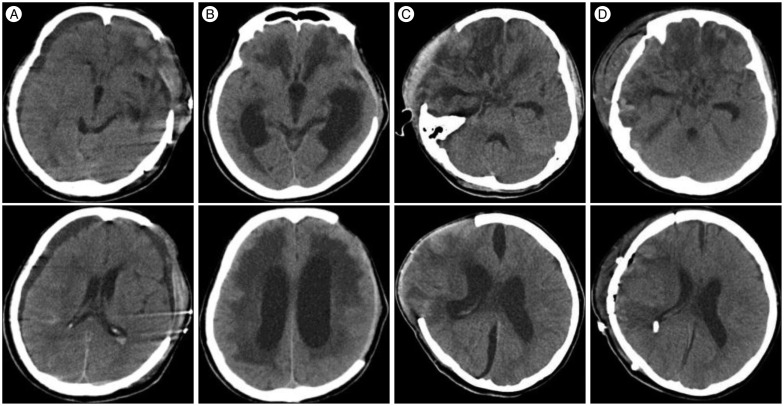
Fig. 2 Computerized tomography (CT) findings of a patient after decompressive craniectomy. A : CT at 12 days after decompressive craniectomy showing contralateral and ipsilateral subdural hygroma. B : CT at 55 days after decompressive craniectomy showed venetriculomagaly and a ventriculo-peritoneal shunt was placed after. C : CT at 28 days after decompressive craniectomy showing interhemispheric subdural hygroma. D : Patient required a ventriculo-peritoneal shunt due to hydrocephalus.
Cited by 1 articles
-
Factors Associated Postoperative Hydrocephalus in Patients with Traumatic Acute Subdural Hemorrhage
Han Kim, Heui Seung Lee, Sung Yeol Ahn, Sung Chun Park, Won Huh
J Korean Neurosurg Soc. 2017;60(6):730-737. doi: 10.3340/jkns.2017.0210.
Reference
-
1. Aarabi B, Chesler D, Maulucci C, Blacklock T, Alexander M. Dynamics of subdural hygroma following decompressive craniectomy : a comparative study. Neurosurg Focus. 2009; 26:E8. PMID: 19485721.2. Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg. 2006; 104:469–479. PMID: 16619648.
Article3. Cardoso ER, Galbraith S. Posttraumatic hydrocephalus--a retrospective review. Surg Neurol. 1985; 23:261–264. PMID: 3975808.
Article4. Cho BR, Lee HJ, Lee HJ, Yi JS, Yang JH, Lee IW. Risk factors for the post-traumatic hydrocephalus following decompressive craniectomy in severe traumatic injury patients. Korean J Neurotrauma. 2012; 8:110–114.
Article5. Choi I, Park HK, Chang JC, Cho SJ, Choi SK, Byun BJ. Clinical factors for the development of posttraumatic hydrocephalus after decompressive craniectomy. J Korean Neurosurg Soc. 2008; 43:227–231. PMID: 19096601.
Article6. Da Costa DG, Adson AW. Subdural hygroma. Arch Surg. 1941; 43:559–567.7. De Bonis P, Pompucci A, Mangiola A, Rigante L, Anile C. Post-traumatic hydrocephalus after decompressive craniectomy : an underestimated risk factor. J Neurotrauma. 2010; 27:1965–1970. PMID: 20812777.
Article8. Dünisch P, Walter J, Sakr Y, Kalff R, Waschke A, Ewald C. Risk factors of aseptic bone resorption : a study after autologous bone flap reinsertion due to decompressive craniotomy. J Neurosurg. 2013; 118:1141–1147. PMID: 23451904.
Article9. Foltz EL, Ward AA Jr. Communicating hydrocephalus from subarachnoid bleeding. J Neurosurg. 1956; 13:546–566. PMID: 13377208.
Article10. Gebel JM, Sila CA, Sloan MA, Granger CB, Weisenberger JP, Green CL, et al. Comparison of the ABC/2 estimation technique to computer-assisted volumetric analysis of intraparenchymal and subdural hematomas complicating the GUSTO-1 trial. Stroke. 1998; 29:1799–1801. PMID: 9731597.
Article11. Greene KA, Marciano FF, Johnson BA, Jacobowitz R, Spetzler RF, Harrington TR. Impact of traumatic subarachnoid hemorrhage on outcome in nonpenetrating head injury. Part I : a proposed computerized tomography grading scale. J Neurosurg. 1995; 83:445–452. PMID: 7666221.
Article12. Honeybul S. Complications of decompressive craniectomy for head injury. J Clin Neurosci. 2010; 17:430–435. PMID: 20181482.
Article13. Honeybul S, Ho KM. Decompressive craniectomy for severe traumatic brain injury : the relationship between surgical complications and the prediction of an unfavourable outcome. Injury. 2014; 45:1332–1339. PMID: 24704150.
Article14. Honeybul S, Ho KM. Incidence and risk factors for post-traumatic hydrocephalus following decompressive craniectomy for intractable intracranial hypertension and evacuation of mass lesions. J Neurotrauma. 2012; 29:1872–1878. PMID: 22583391.
Article15. Honeybul S, Ho KM. Long-term complications of decompressive craniectomy for head injury. J Neurotrauma. 2011; 28:929–935. PMID: 21091342.
Article16. Huh PW, Yoo DS, Cho KS, Park CK, Kang SG, Park YS, et al. Diagnostic method for differentiating external hydrocephalus from simple subdural hygroma. J Neurosurg. 2006; 105:65–70. PMID: 16874890.
Article17. Jeon SW, Choi JH, Jang TW, Moon SM, Hwang HS, Jeong JH. Risk factors associated with subdural hygroma after decompressive craniectomy in patients with traumatic brain injury : a comparative study. J Korean Neurosurg Soc. 2011; 49:355–358. PMID: 21887394.
Article18. Kaen A, Jimenez-Roldan L, Alday R, Gomez PA, Lagares A, Alén JF, et al. Interhemispheric hygroma after decompressive craniectomy : does it predict posttraumatic hydrocephalus? J Neurosurg. 2010; 113:1287–1293. PMID: 20486895.
Article19. Kilincer C, Simsek O, Hamamcioglu MK, Hicdonmez T, Cobanoglu S. Contralateral subdural effusion after aneurysm surgery and decompressive craniectomy : case report and review of the literature. Clin Neurol Neurosurg. 2005; 107:412–416. PMID: 16023537.
Article20. Lee KS. The pathogenesis and clinical significance of traumatic subdural hygroma. Brain Inj. 1998; 12:595–603. PMID: 9653522.
Article21. Marmarou A, Foda MA, Bandoh K, Yoshihara M, Yamamoto T, Tsuji O, et al. Posttraumatic ventriculomegaly : hydrocephalus or atrophy? A new approach for diagnosis using CSF dynamics. J Neurosurg. 1996; 85:1026–1035. PMID: 8929491.
Article22. Murata K. Chronic subdural hematoma may be preceded by persistent traumatic subdural effusion. Neurol Med Chir (Tokyo). 1993; 33:691–696. PMID: 7505896.
Article23. Ohno K, Suzuki R, Masaoka H, Matsushima Y, Inaba Y, Monma S. Chronic subdural haematoma preceded by persistent traumatic subdural fluid collection. J Neurol Neurosurg Psychiatry. 1987; 50:1694–1697. PMID: 3437306.
Article24. Rahme R, Weil AG, Sabbagh M, Moumdjian R, Bouthillier A, Bojanowski MW. Decompressive craniectomy is not an independent risk factor for communicating hydrocephalus in patients with increased intracranial pressure. Neurosurgery. 2010; 67:675–678. discussion 678PMID: 20651634.
Article25. Stiver SI. Complications of decompressive craniectomy for traumatic brain injury. Neurosurg Focus. 2009; 26:E7. PMID: 19485720.
Article26. Su TM, Lee TH, Huang YH, Su FW, Chen WF. Contralateral subdural effusion after decompressive craniectomy in patients with severe traumatic brain injury : clinical features and outcome. J Trauma. 2011; 71:833–837. PMID: 21610528.
Article27. Vanneste J, Augustijn P, Davies GA, Dirven C, Tan WF. Normal-pressure hydrocephalus. Is cisternography still useful in selecting patients for a shunt? Arch Neurol. 1992; 49:366–370. PMID: 1558516.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk Factors for the Post-Traumatic Hydrocephalus Following Decompressive Craniectomy in Severe Traumatic Injury Patients
- Risk Factors Associated with Subdural Hygroma after Decompressive Craniectomy in Patients with Traumatic Brain Injury : A Comparative Study
- Paradoxical Herniation after Decompressive Craniectomy for Acute Subdural Hematoma
- "Syndrome of the Sinking Skin-Flap" Secondary to the Ventriculoperitoneal Shunt after Craniectomy
- Chronic Subdural Hematoma Superimposed on Posttraumatic Subdural Hygroma: A Report of Three Cases
