Locations and Clinical Significance of Non-Hemorrhagic Brain Lesions in Diffuse Axonal Injuries
- Affiliations
-
- 1Department of Neurosurgery, Chung-Ang University Hospital, Seoul, Korea. cuttage@cau.ac.kr
- KMID: 2190656
- DOI: http://doi.org/10.3340/jkns.2012.52.4.377
Abstract
OBJECTIVE
Detection of focal non-hemorrhagic lesion (NHL) has become more efficient in diffuse axonal injury (DAI) patients using an MRI. The aims of this study are to find out the radiological distribution, progress of NHL and its clinical significance.
METHODS
Between September 2005 and October 2011, 32 individuals with NHLs on brain MRI were enrolled. NHLs were classified by brain location into 4 major districts and 13 detailed locations including cortical and subcortical, corpus callosum, deep nuclei and adjacent area, and brainstem. The severity of NHL was scored from grades 1 to 4, according to the number of districts involved. Fourteen patients with NHL were available for MRI follow-up and an investigation of the changes was conducted.
RESULTS
Thirty-two patients had 59 NHLs. The most common district of NHL was cortical and subcortical area; 15 patients had 20 NHSs. However the most common specific location was the splenium of the corpus callosum; 14 patients had 14 lesions. The more lesions patients had, the lower the GCS, however, this was not a statistically meaningful difference. On follow-up MRI in 14 patients, out of 24 lesions, 13 NHLs resolved, 5 showed cystic change, and 6 showed atrophic changes.
CONCLUSION
NHLs were located most commonly in the splenium and occur frequently in the thalamus and the mesial temporal lobe. Because most NHS occur concomitantly with hemorrhagic lesions, it was difficult to determine their effects on prognosis. Since most NHLs resolve completely, they are probably less significant to prognosis than hemorrhagic lesions.
Keyword
MeSH Terms
Figure
-
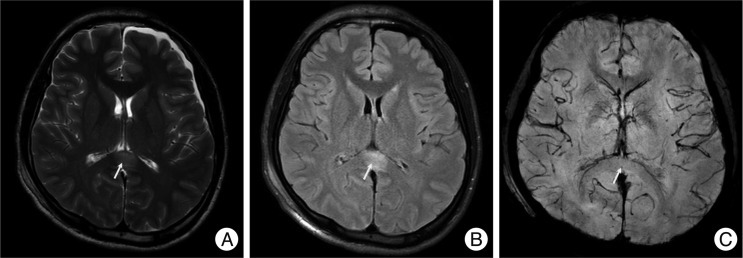
Fig. 1 A non-hemorrhagic lesion of the corpus callosum. A 21-year-old male was admitted due to a bicycle accident. Upon admission his Glasgow coma scale score was 6 points. MRI shows a non-hemorrhagic lesion (arrows) at the splenium of the corpus callosum. Non-hemorrhagic lesions show high signal intensity at T2W1 (A) and FLAIR (B), but dark signals cannot be seen on SWI (C).
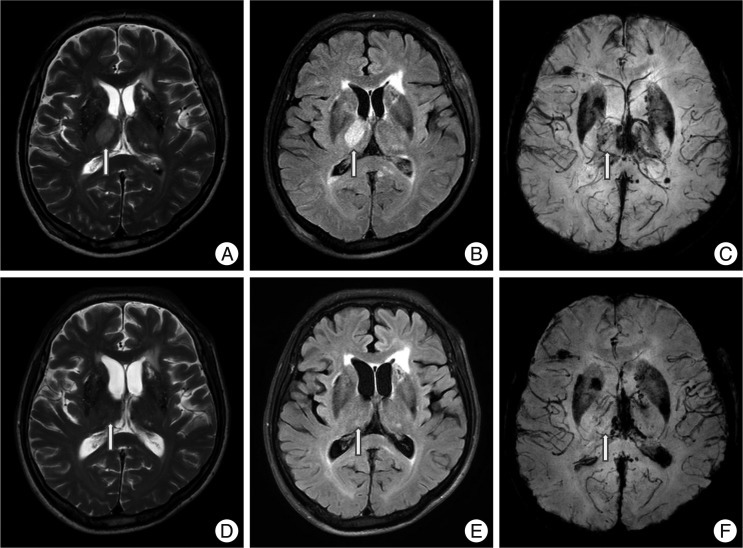
Fig. 2 A non-hemorrhagic lesion of the thalamus area. A 57-year-old male was admitted due to a pedestrian car accident, with a Glasgow coma scale of 7 on admission. MRI shows a non-hemorrhagic lesion at the right thalamus (arrow). Non-hemorrhagic lesions show high signal intensity at T2W1 (A) and FLAIR (B), but a dark signal cannot be seen on SWI (C). However, at one month follow-up, the previous high signal at T2W1 (D), FLAIR (E) is not seen and SWI (F) still showed no dark signals.
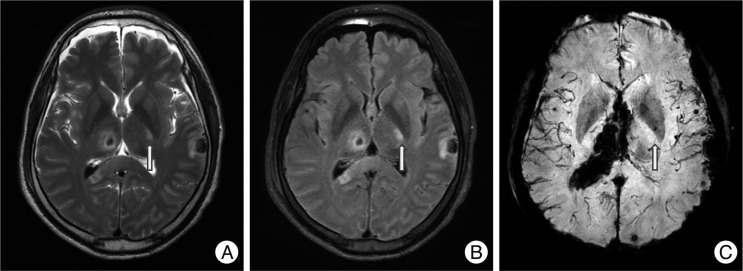
Fig. 3 A non-hemorrhagic lesion of the internal capsule. A 45-year-old male fell and was admitted to the emergency room. His initial Glasgow coma scale was 4 points and he was in a semi-coma. MRI shows a non-hemorrhagic lesion in the left internal capsule posterior limb at T2W1 (arrow, A) and FLAIR (B) with no dark signal at SWI (C). Hemorrhagic lesions are also noted in the corpus callosum, thalamus, brainstem and cerebellum.
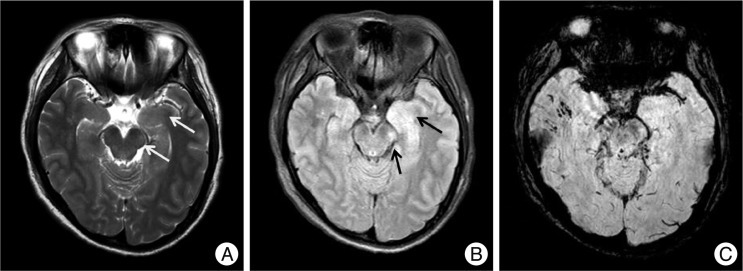
Fig. 4 Non-hemorrhagic lesions of the brainstem and hippocampus. A 35-year-old woman was admitted in a semicomatose state after a fall. T2WI (A) and FLAIR (B) shows a bright dot on the left crus cerebri of the midbrain (arrows) and SWI (C) does not show low signal intensity. Another non-hemorrhagic lesion is suspected on the left hippocampus. FLAIR (B) shows a bright signal intensity lesion from the left pes hippocampus to the body of the hippocampus, which is not prominent on T2WI (A) except slightly swollen pes hippocampus. Several petechial hemorrhagic lesions are also noted in the right temporal subcortical area and left mesial temporal area.
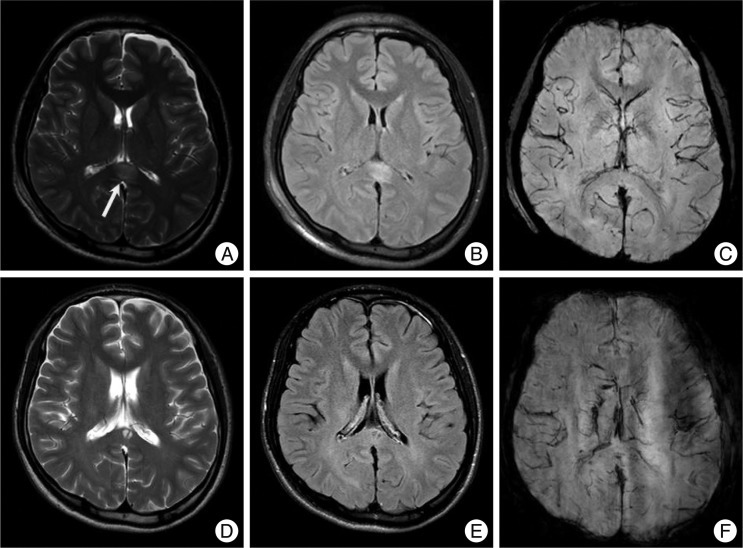
Fig. 5 Cystic changes of non-hemorrhagic lesions on the corpus callosum. A 22-year-old man with a splenial non-hemorrhagic lesion (arrow, A : T2WI, B : FLAIR, C : SWI). Follow-up images in three months show a small cyst on the same area of splenium (D : T2WI, E : FLAIR, F : SWI).
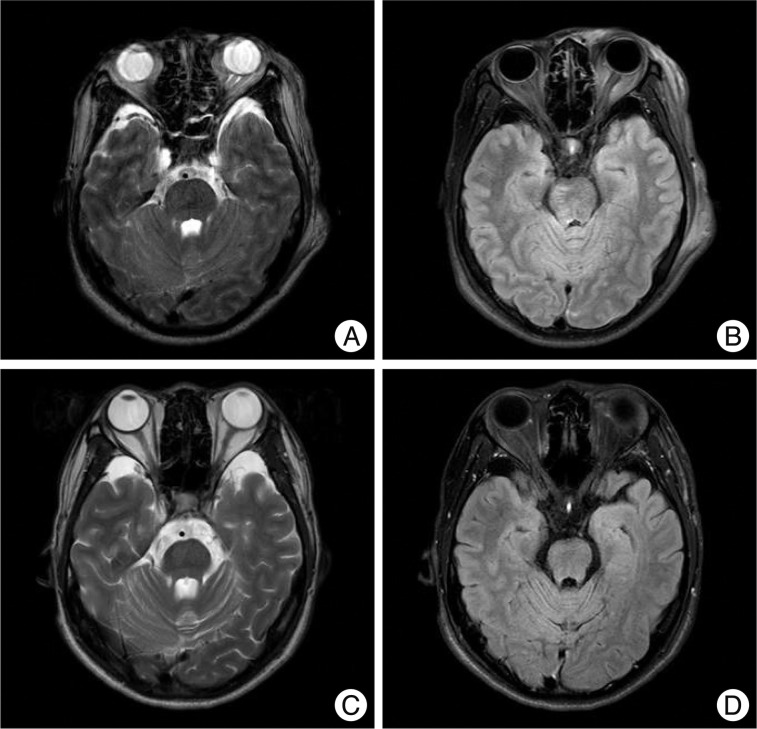
Fig. 6 Atrophy of non-hemorrhagic lesion on brainstem. A 34-year-old man with a lesion on the right dorso-ventral midbrain. Follow-up images at two years show no abnormal signal in the midbrain, however, the volume of the midbrain seems to be smaller than the initial images especially on the right side (A : initial T2WI, B : initial FLAIR, C : 2-year follow-up T2WI, D : 2-year follow-up FLAIR).
Reference
-
1. Adams JH. Diffuse axonal injury in non-missile head injury. Injury. 1982; 13:444–445. PMID: 7085064.
Article2. Adams JH. The autopsy in fatal non-missile head injuries. Curr Top Pathol. 1988; 76:1–22. PMID: 3286136.
Article3. Adams JH, Doyle D, Ford I, Gennarelli TA, Graham DI, McLellan DR. Diffuse axonal injury in head injury : definition, diagnosis and grading. Histopathology. 1989; 15:49–59. PMID: 2767623.4. Adams H, Mitchell DE, Graham DI, Doyle D. Diffuse brain damage of immediate impact type. Its relationship to 'primary brain-stem damage' in head injury. Brain. 1977; 100:489–502. PMID: 589428.5. Ezaki Y, Tsutsumi K, Morikawa M, Nagata I. Role of diffusion-weighted magnetic resonance imaging in diffuse axonal injury. Acta Radiol. 2006; 47:733–740. PMID: 16950714.
Article6. Gennarelli TA, Thibault LE, Adams JH, Graham DI, Thompson CJ, Marcincin RP. Diffuse axonal injury and traumatic coma in the primate. Ann Neurol. 1982; 12:564–574. PMID: 7159060.
Article7. Gentry LR, Godersky JC, Thompson BH. Traumatic brain stem injury : MR imaging. Radiology. 1989; 171:177–187. PMID: 2928523.8. Gentry LR, Thompson B, Godersky JC. Trauma to the corpus callosum : MR features. AJNR Am J Neuroradiol. 1988; 9:1129–1138. PMID: 3143234.9. Grcević N. The concept of inner cerebral trauma. Scand J Rehabil Med Suppl. 1988; 17:25–31. PMID: 3041565.10. Haacke EM, Xu Y, Cheng YC, Reichenbach JR. Susceptibility weighted imaging (SWI). Magn Reson Med. 2004; 52:612–618. PMID: 15334582.
Article11. Hardman JM. The pathology of traumatic brain injuries. Adv Neurol. 1979; 22:15–50. PMID: 384769.12. Komatsu S, Sato T, Kagawa S, Mori T, Namiki T. Traumatic lesions of the corpus callosum. Neurosurgery. 1979; 5:32–35. PMID: 471202.
Article13. Kubal WS. Updated imaging of traumatic brain injury. Radiol Clin North Am. 2012; 50:15–41. PMID: 22099485.
Article14. Le TH, Gean AD. Winn HR, editor. Radiology of traumatic brain injury. Youman's Neurological Surgery. 2011. Vol 4. Philadeophia: Elsevier;p. 3342–3361.15. Lindenberg R. Significance of the tentorium in head injuries from blunt forces. Clin Neurosurg. 1964; 12:129–142. PMID: 5865035.
Article16. Lindenberg R, Fisher RS, Durlacher SH, Lovitt WV Jr, Freytag E. Lesions of the corpus callosum following blunt mechanical trauma to the head. Am J Pathol. 1955; 31:297–317. PMID: 14350067.17. Lindenberg R, Freytag E. The mechanism of cerebral contusions. A pathologic-anatomic study. Arch Pathol. 1960; 69:440–469. PMID: 14417116.18. Maxwell WL, Povlishock JT, Graham DL. A mechanistic analysis of nondisruptive axonal injury : a review. J Neurotrauma. 1997; 14:419–440. PMID: 9257661.19. Meaney DF, Margulies SS, Smith DH. Diffuse axonal injury. J Neurosurg. 2001; 95:1108–1110. PMID: 11765833.20. Peerless SJ, Rewcastle NB. Shear injuries of the brain. Can Med Assoc J. 1967; 96:577–582. PMID: 6020206.21. Povlishock JT. Pathophysiology of neural injury : therapeutic opportunities and challenges. Clin Neurosurg. 2000; 46:113–126. PMID: 10944671.22. Povlishock JT. Traumatically induced axonal injury : pathogenesis and pathobiological implications. Brain Pathol. 1992; 2:1–12. PMID: 1341941.23. Povlishock JT, Christman CW. The pathobiology of traumatically induced axonal injury in animals and humans : a review of current thoughts. J Neurotrauma. 1995; 12:555–564. PMID: 8683606.
Article25. Strich SJ. Diffuse degeneration of the cerebral white matter in severe dementia following head injury. J Neurol Neurosurg Psychiatry. 1956; 19:163–185. PMID: 13357957.
Article26. Strich SJ. Lesions in the cerebral hemispheres after blunt head injury. J Clin Pathol Suppl (R Coll Pathol). 1970; 4:166–171. PMID: 4123922.
Article27. Tong KA, Ashwal S, Holshouser BA, Shutter LA, Herigault G, Haacke EM, et al. Hemorrhagic shearing lesions in children and adolescents with posttraumatic diffuse axonal injury : improved detection and initial results. Radiology. 2003; 227:332–339. PMID: 12732694.
Article28. Topal NB, Hakyemez B, Erdogan C, Bulut M, Koksal O, Akkose S, et al. MR imaging in the detection of diffuse axonal injury with mild traumatic brain injury. Neurol Res. 2008; 30:974–978. PMID: 18691451.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MRI of the diffuse axonal injury
- The MRI Findings and Clinical Analysis in the Severe Diffuse Axonal Injury
- Comparison of brain MRI and CT of diffuse axonal injury(DIA)
- Time to Recover Consciousness in Patients with Diffuse Axonal Injury : Assessment with Reference to Magnetic Resonance Grading
- Diagnostic History of Traumatic Axonal Injury in Patients with Cerebral Concussion and Mild Traumatic Brain Injury
