J Korean Assoc Oral Maxillofac Surg.
2011 Feb;37(1):72-76. 10.5125/jkaoms.2011.37.1.72.
Polymorphous low-grade adenocarcinoma on hard palate: case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Kyungpook National University, Daegu, Korea. cskim@knu.ac.kr
- 2Department of Dentistry, Ulsan University Hospital, Ulsan, Korea.
- KMID: 2189810
- DOI: http://doi.org/10.5125/jkaoms.2011.37.1.72
Abstract
- Polymorphous low-grade adenocarcinomas (PLGA) are distinctive salivary gland neoplasms with a propensity to arise from the minor salivary glands. The most frequent location of PLGA is the palate, even though other locations have been described. Previously used terms for PLGA include lobular carcinoma and terminal duct carcinoma. Although the frequency of the tumor is unknown, the recognition of PLGA as an individual tumor has increased with the establishment of specific histopathological criteria characterizing the PLGA. The first choice of treatment is a wide surgical excision including the subjacent bone if necessary. The prognosis is generally good and the recurrence rate ranges from 17% and 22%. Distant metastases is unusual (9%) but occur mainly in the regional lymph nodes. This is a case report of a 67 year old female patient with PLGA who was treated with a wide excision by layers (2 stage) of the lesion including the surrounding bone. We present this case with a review of the relevant literature.
MeSH Terms
Figure
-

Fig. 1. Ulcerative lesion on right palate was showed at first visit.
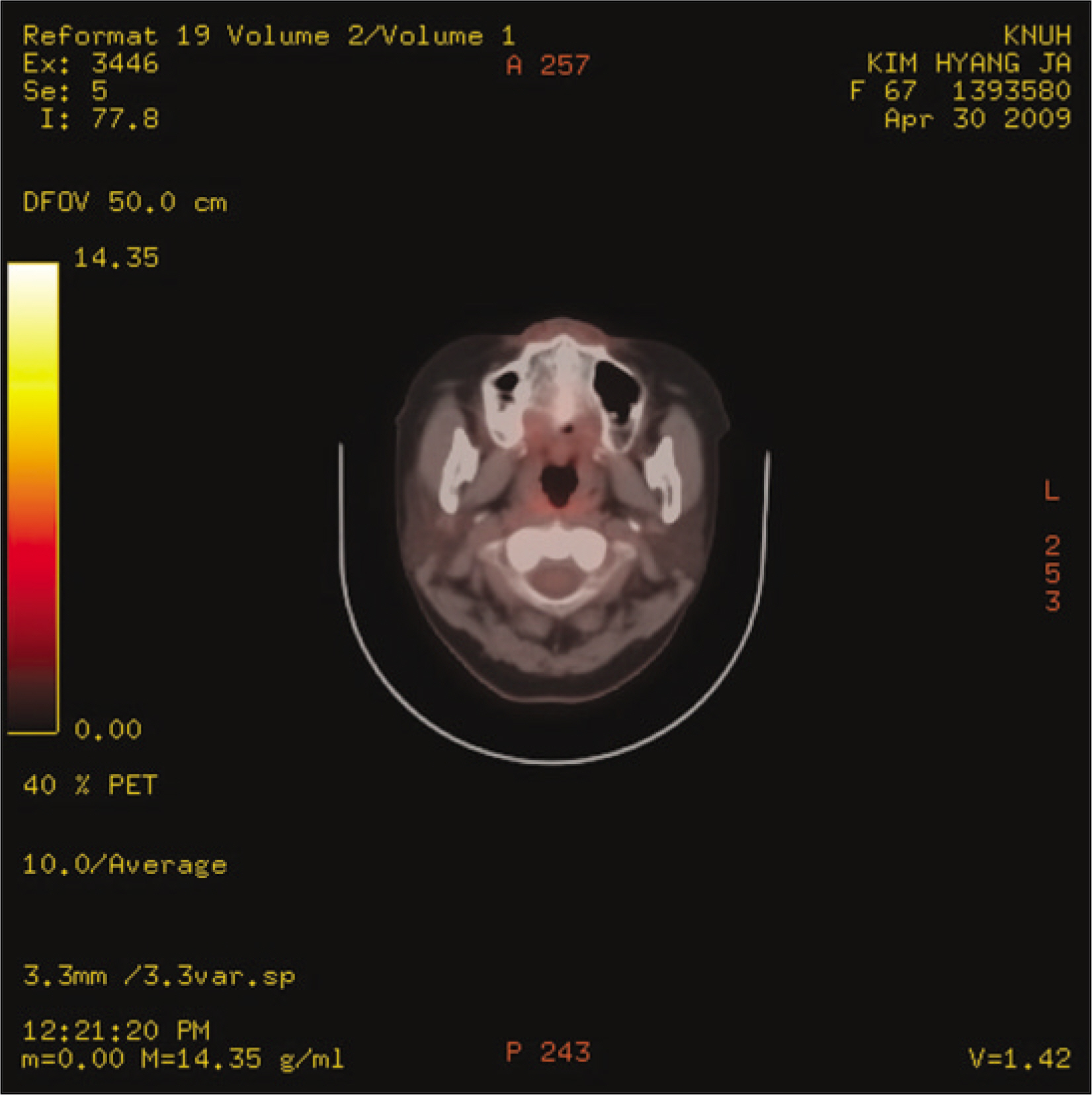
Fig. 2. PET-CT: without significant focal FDG uptake in right palate.(PET-CT: positron emission tomography-computed tomography, FDG: fluorodeoxyglucose)

Fig. 3. Excised mass of tumor and underlying bone.

Fig. 4. Intraoral view of postoperation state.

Fig. 5. Ten months after surgery: operation site is unremarkable.
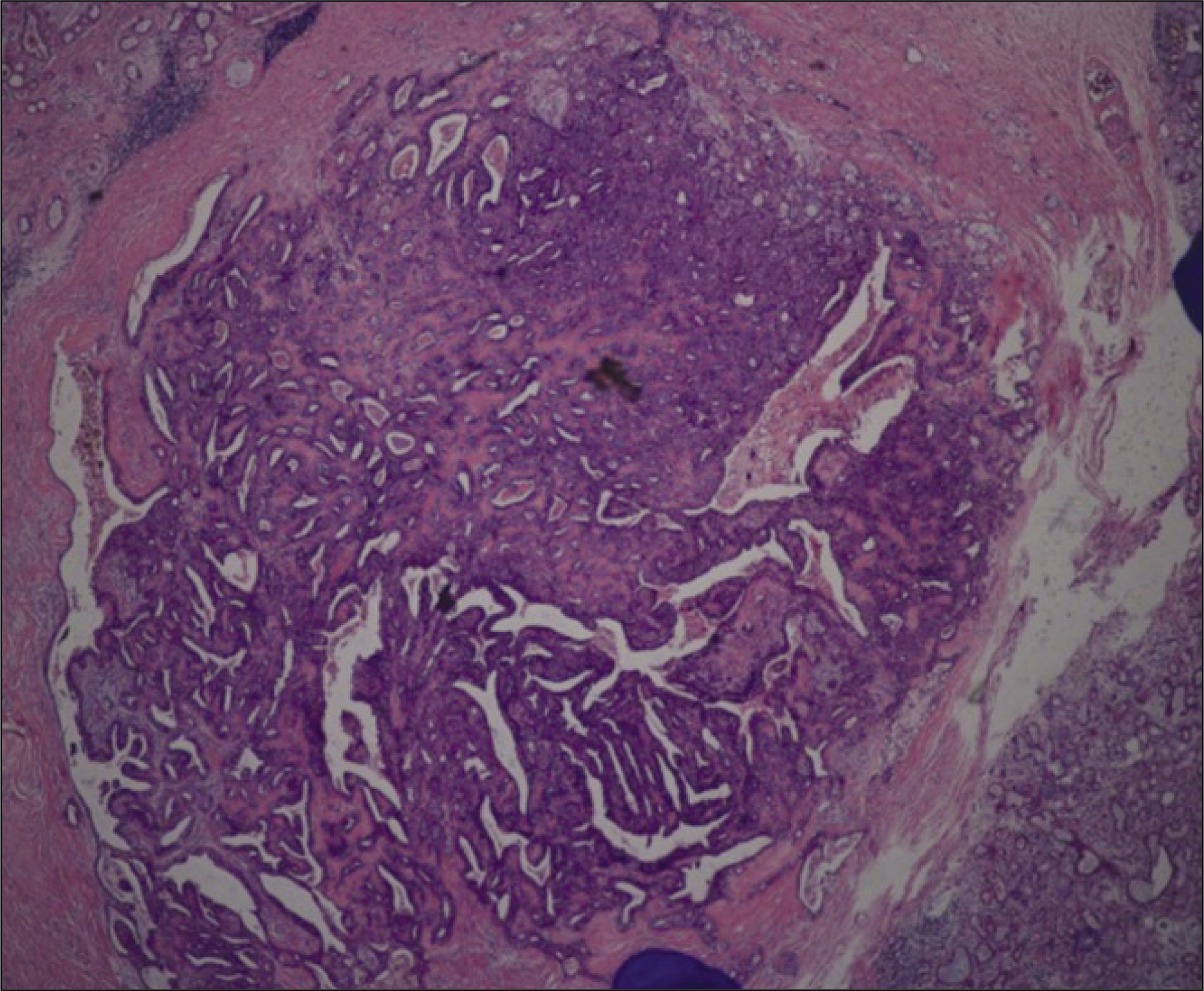
Fig. 6. Histological overview.(H&E staining, original magnification 4×10)
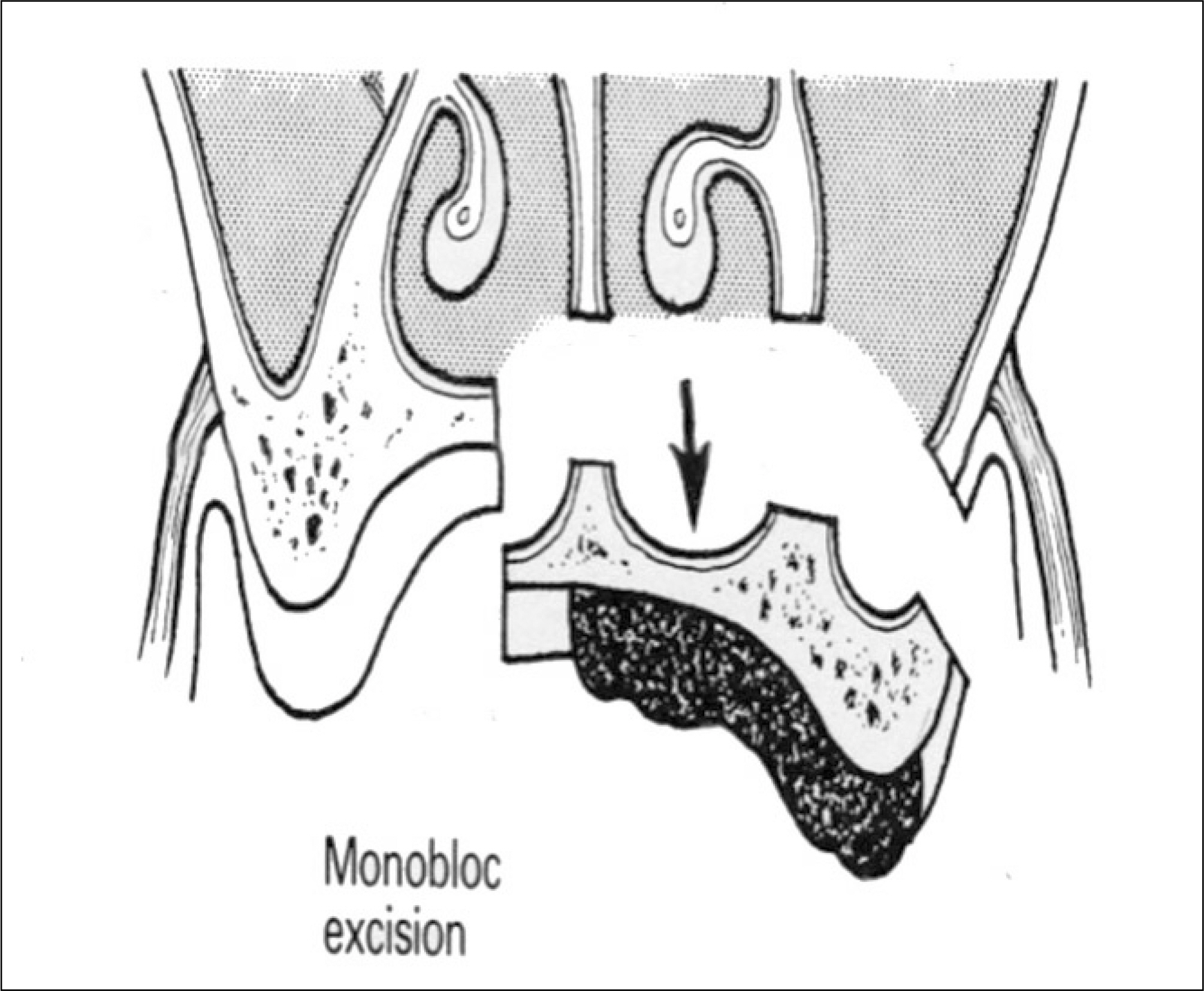
Fig. 7. Schematic view of monobloc excision.
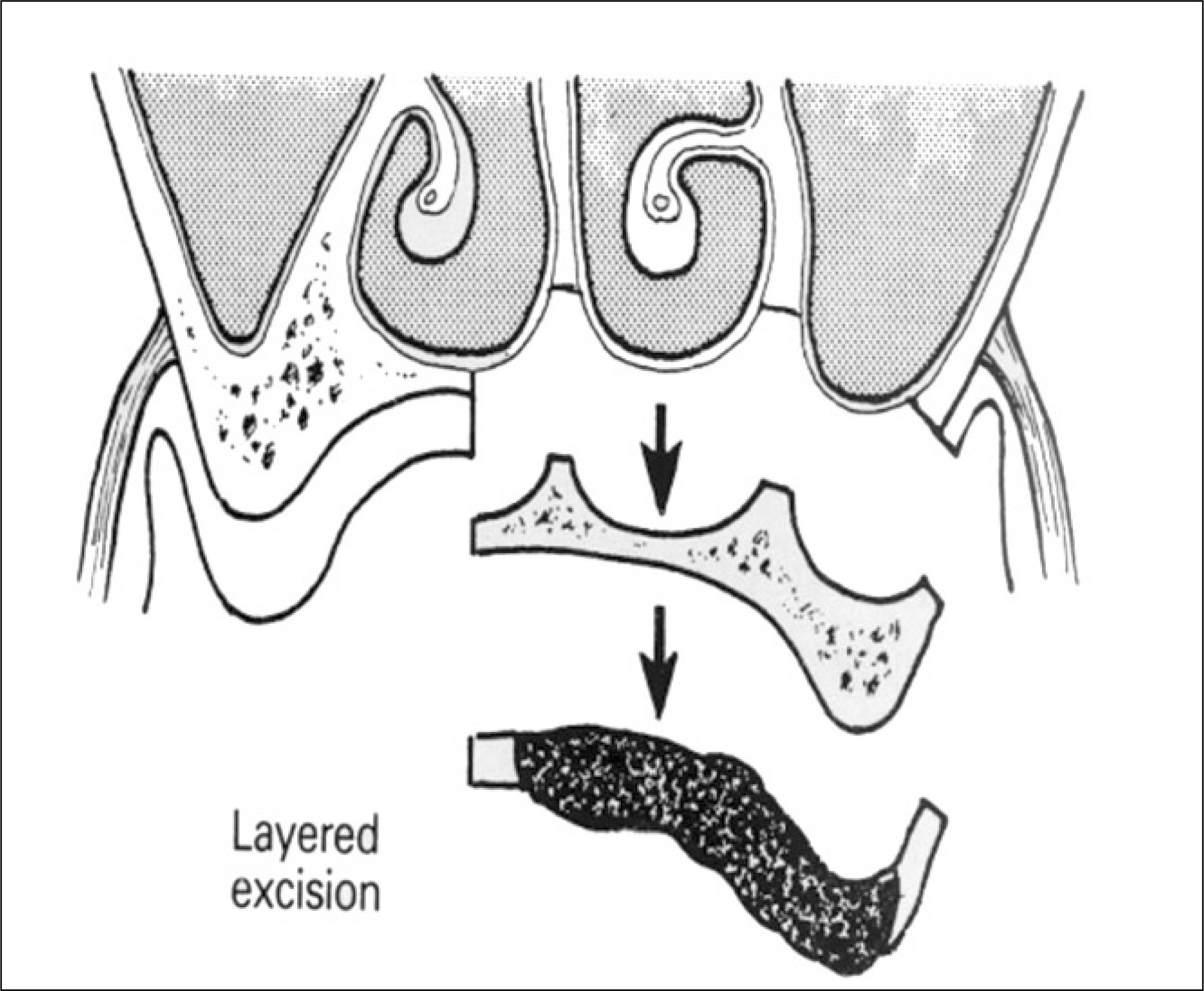
Fig. 8. Schematic view of excision by layers.

Fig. 9. Postoperative Water's view.
Reference
-
References
1. Furuse C, Tucci R, Machado de Sousa SO, Rodarte Carvalho Y, Cavalcanti de Arau ′ jo V. Comparative immunoprofile of polymorphous low-grade adenocarcinoma and canalicular adenoma. Ann Diagn Pathol. 2003; 7:278–80.
Article2. Freedman PD, Lumerman H. Lobular carcinoma of intraoral minor salivary gland origin. Report of twelve cases. Oral Surg Oral Med Oral Pathol. 1983; 56:157–66.3. Frierson HF Jr, Mills SE, Garland TA. Terminal duct carcinoma of minor salivary glands. A nonpapillary subtype of polymorphous low-grade adenocarcinoma. Am J Clin Pathol. 1985; 84:8–14.
Article4. Castle JT, Thompson LD, Frommelt RA, Wenig BM, Kessler HP. Polymorphous low grade adenocarcinoma: a clinicopathologic study of 164 cases. Cancer. 1999; 86:207–19.5. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and maxillofacial pathology. 2nd ed.Philadelphia: WB Saunders;2002.6. Clayton JR, Pogrel MA, Regezi JA. Simultaneous multifocal polymorphous low-grade adenocarcinoma. Report of two cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 80:71–7.7. Kelsch RD, Bhuiya T, Fuchs A, Gentile P, Kahn MA, Fantasia JE. Polymorphous low-grade adenocarcinoma: flow cytometric, p53, and PCNA analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 84:391–9.8. Darling MR, Schneider JW, Phillips VM. Polymorphous low-grade adenocarcinoma and adenoid cystic carcinoma: a review and comparison of immunohistochemical markers. Oral Oncol. 2002; 38:641–5.
Article9. Curran AE, White DK, Damm DD, Murrah VA. Polymorphous low-grade adenocarcinoma versus pleomorphic adenoma of minor salivary glands: resolution of a diagnostic dilemma by immunohistochemical analysis with glial fibrillary acidic protein. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 91:194–9.
Article10. Miliauskas JR. Polymorphous low-grade (terminal duct) adenocarcinoma of the parotid gland. Histopathology. 1991; 19:555–7.
Article11. Haba R, Kobayashi S, Miki H, Hirakawa E, Saoo K, Iwai T, et al. Polymorphous low-grade adenocarcinoma of submandibular gland origin. Acta Pathol Jpn. 1993; 43:774–8.
Article12. Blanchaert RH, Ord RA, Kumar D. Polymorphous low-grade adenocarcinoma of the sublingual gland. Int J Oral Maxillofac Surg. 1998; 27:115–7.
Article13. de Diego JI, Bernaldez R, Prim MP, Hardisson D. Polymorphous low-grade adenocarcinoma of the tongue. J Laryngol Otol. 1996; 110:700–3.
Article14. Kumar M, Stivaros N, Barrett AW, Thomas GJ, Bounds G, Newman L. Polymorphous low-grade adenocarcinoma-a rare and aggressive entity in adolescence. Br J Oral Maxillofac Surg. 2004; 42:195–9.
Article15. Mills SE, Garland TA, Allen MS Jr. Low-grade papillary adenocarcinoma of palatal salivary gland origin. Am J Surg Pathol. 1984; 8:367–74.
Article16. Simpson RH, Pereira EM, Ribeiro AC, Abdulkadir A, Reis-Filho JS. Polymorphous low-grade adenocarcinoma of the salivary glands with transformation to high-grade carcinoma. Histopathology. 2002; 41:250–9.
Article17. Pelkey TJ, Mills SE. Histologic transformation of polymorphous low-grade adenocarcinoma of salivary gland. Am J Clin Pathol. 1999; 111:785–91.
Article18. Gibbons D, Saboorian MH, Vuitch F, Gokaslan ST, Ashfaq R. Fine-needle aspiration findings in patients with polymorphous low grade adenocarcinoma of the salivary glands. Cancer. 1999; 87:31–6.
Article19. Gnepp DR, el-Mofty S. Polymorphous low-grade adenocarcinoma: glial fibrillary acidic protein staining in the differential diagnosis with cellular mixed tumors. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 83:691–5.20. McGregor IA, McGregor FM. Cancer of the face and mouth: pathology and management for surgeons. New York: Churchill Livingstone;1986.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fine Needle Aspiraton Cytology of Polymorphous Low Grade Adenocarcinoma in the Hard Palate: A Case Report
- Polymorphous Low-Grade Adenocarcinoma in the Nasopharynx: A Case Report and Review of the Literature
- A Case of Polymorphous Low Grade Adenocarcinoma in Submandibular Gland
- Polymorphous Low-grade Adenocarcinoma of the Palate: Case Report
- A Case of Polymorphous Low Grade Adenocarcinoma Arising from Warthin's Tumor
