Imaging Diagnosis of Asbestosis
- Affiliations
-
- 1Department of Radiology, Dongguk University College of Medicine, Korea. jeungkim@duih.org, kjs7143@kornet.net
- KMID: 2188007
- DOI: http://doi.org/10.5124/jkma.2009.52.5.465
Abstract
- Asbestosis is diffuse interstitial pulmonary fibrosis associated with asbestos fiber inhalation. The typical chest radiographic findings in asbestosis are small irregular or reticular opacities, predominating at the lung bases. Honeycombing is evident in more advanced diseases. But chest radiograph is relatively insensitive in detecting the presence of asbestosis. HRCT is more sensitive than simple chest radiograph for diagnosis of asbestosis, especially the early change of asbestosis. The early findings of asbestosis on HRCT are subpleural dotlike opacities and curvilinear opacities. As progression of fibrosis, intralobular interstitial thickening and interlobular septal thickening are presented. In advanced diseases, parenchymal bands, traction bronchiectasis or bronchiolectasis, and honeycombing are noted. These findings are typically located in lower posterior subpleural portions with bilateral symmetric patterns. Imaging findings that are compatible with asbestosis, rale, and a reduced diffusing capacity can increase confidence of diagnosis of asbestosis.
Keyword
MeSH Terms
Figure
-

Figure 1 A 71-year-old woman with asbestosis. (A) Chest PA radiograph shows reticular and small nodular densities in both lungs, more prominent in lower lungs. And multiple calcified plaques are also seen in both mid thoraces and both diaphragmatic pleura. (B) Magnification view of left lung shows reticular densities and small nodular densities.
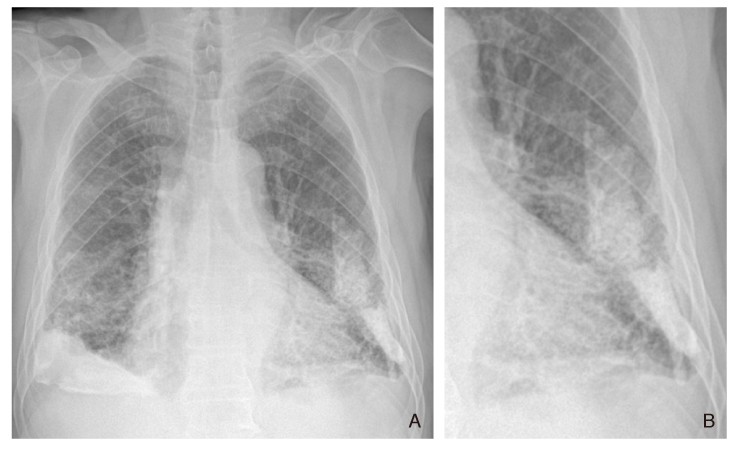
Figure 2 A 80-year-old man with asbestosis. (A) Chest PA radiograph shows reticular densities and honeycombing in both lungs, more prominent in lower lungs with bilateral symmetric distribution. And multiple dense calcified plaques are seen in both lower thoraces and both diaphragmatic pleura. (B) Magnification view of left lung shows reticular densities and honeycombings.
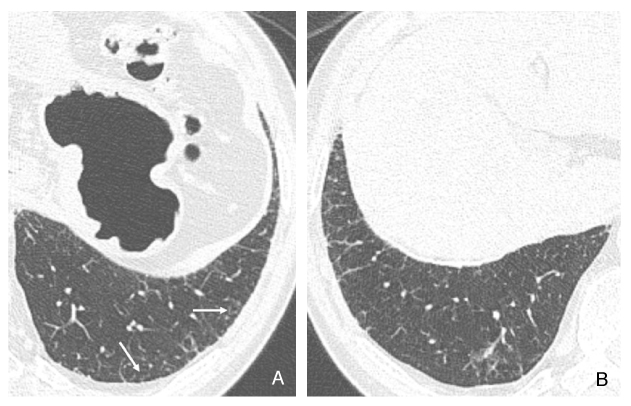
Figure 3 A 75-year-old man with asbestosis. (A) HRCT shows dotlike opacities associated with intralobular interstitial thickening in the subpleural lung (arrows). (B) HRCT shows reticular patterns in the lung periphery corresponding to thickened interlobular septa.
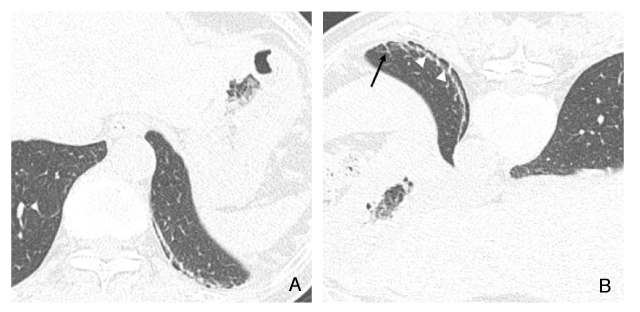
Figure 4 A 77-year-old woman with asbestosis. (A) Supine HRCT shows a curvilinear line in the posterior left lung. (B) Prone HRCT shows a subpleural line (white arrowheads) and a parenchymal band (black arrow).
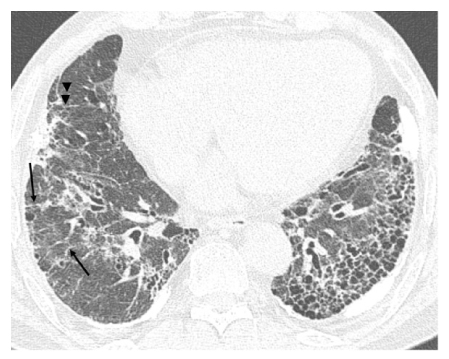
Figure 5 A 80-year-old man with asbestos exposure with pleural thickening and calcification. HRCT shows extensive honeycombing at the left lung base. Interlobular septal thickening (arrows) and parenchymal band (arrowheads) are also noted in right lung.

Figure 6 Dependent atelectasis in a patient with asbestos exposure. (A) In the supine HRCT, focal ill-defined ground-glass opacity (GGO) and short line are visible posteriorly. (B) In the prone HRCT, the lungs are normal in appearance. There is no evidence of GGO and fibrosis.
Reference
-
1. Kim JS, Lynch DA. Imaging of nonmalignant occupational lung disease. J Thorac Imaging. 2002. 17:238–260.
Article2. McLoud TC. Conventional radiography in the diagnosis of asbestos-related disease. Radiol Clin North Am. 1992. 30:1177–1189.3. Lynch DA, Gamsu G, Ray CS, Aberle DR. Asbestos-related focal lung masses: manifestations on conventional and high-resolution CT scans. Radiology. 1988. 169:603–607.
Article4. Gefter WB, Conant EF. Issues and controversies in the plain-film diagnosis of asbestos-related disorders in the chest. J Thorac Imaging. 1988. 3:11–28.
Article5. Gefter WB, Epstein D, Miller W. Radiographic evaluation of asbestos- related chest disorders. Crit Rev Diagn Imaging. 1984. 21:123–181.6. American Thoracic Society. The diagnosis of nonmalignant diseases related to asbestos. Am Rev Respir Dis. 1986. 134:363–368.
Article7. Gaensler EA, Jederlinic PJ, Churg A. Idiopathic pulmonary fibrosis in asbestos-exposed workers (see comments). Am Rev Respir Dis. 1991. 144:477–478.8. Kipen HM, Lilis R, Suzuki Y, Valciukas JA, Selikoff IJ. Pulmonary fibrosis in asbestos insulation workers with lung cancer: a radiological and histopathological evaluation. Br J Ind Med. 1987. 44:96–100.
Article9. Epler GR, McLoud TC, Gaensler EA, Mikus JP, Carrington CB. Normal chest roent-genograms in chronic diffuse infiltrative lung disease. N Engl J Med. 1978. 298:934–939.
Article10. Klass VE. A diagnositic approach to asbestosis, utilizing clinical criteria, high resolution computed tomonography, and gallium scanning. Am J Ind Med. 1993. 23:801–809.11. Webb WR, Muller NL, Naidich DP. Kluwer W, editor. Pneumoconiosis, occupational, and environmental lung disease. High-resolution CT of the lung. 2009. 3rd ed. Philadelphia: Lippincott Williams & Wilkins;301–334.12. Akira M, Yamamoto S, Inoue Y, Sakatani M. High-resolution CT of asbestosis and idiopathic pulmonary fibrosis. AJR Am J Roentgenol. 2003. 181:163–169.
Article13. Akira M, Yokoyama K, Yamamoto S, Higashihara T, Morinaga K, Kita N, Morimoto S, Ikezoe J, Kozuka T. Early asbestosis: evaluation with high-resolution CT. Radiology. 1991. 178:409–416.
Article14. Aberle DR, Gamsu G, Ray CS, Feuerstein IM. Asbestos-related pleural and parenchymal fibrosis: detection with high-resolution CT. Radiology. 1988. 166:729–734.
Article15. Aberle DR, Gamsu G, Ray CS. High-resolution CT of benign asbestos-related diseases: clinical and radiographic correlation. AJR Am J Roentgenol. 1988. 151:883–891.
Article16. Akira M, Yamamoto S, Yokoyama K, Kita N, Morinaga K, Higashihara T, Kozuka T. Asbestosis: high-resolution CT-pathologic correlation. Radiology. 1990. 176:389–394.
Article17. Parks WR. Parks WR, editor. An approach to the differential diagnosis of asbestosis and non-occupational diffuse interstitial pulmonary fibrosis. Occupational lung disorders. 1994. 3rd ed. London: Butterworth-Heinemann;505–535.18. al Jarad N, Strickland B, Pearson MC, Rubens MB, Rudd RH. High-resolution computed tomographic assessment of asbestosis and cryp-togenic fibrosing alveolitis: a comparative study. Thorax. 1992. 47:645–650.
Article19. Copley SJ, Wells AU, Sivakumaran P, Rubens MB, Lee YCG, Desai SR, MacDonald SLS, Thomson RI, Colby TV, Nicholson AG, du Bois RM, Musk AW, Hansell DM. Asbestosis and idiopathic pulmonary fibrosis: comparison of thin-section CT features. Radiology. 2003. 229:731–736.
Article20. Staples CA, Gamsu G, Ray CS, Webb WR. High resolution computed tomography and lung function in asbestos-exposed workers with normal chest radiographs. Am Rev Respir Dis. 1989. 139:1502–1508.
Article21. Friedman AC, Fiel SB, Radecki PD, Lev-Toaff AS. Computed tomog raphy of benign pleural and pulmonary parenchymal abnor-malities related to asbestos exposure. Semin Ultrasound CT MR. 1990. 11:393–408.22. Friedman AC, Fiel SB, Fisher MS, Radecki PD, Lev-Toaff AS, Cardine DF. Asbestos-related pleu-ral disease and asbestosis: a comparison of CT and chest radi-ography. AJR Am J Roentgenol. 1988. 150:269–275.
Article23. Gamsu G, Salmon CJ, Warnock ML, Blanc PD. CT quantification of interstitial fibrosis in patients with asbestosis: a comparison of two methods. AJR Am J Roentgenol. 1995. 164:63–68.
Article24. Ross RM. The clinical diagnosis of asbestosis in this century requires more than a chest radiograph. Chest. 2003. 124:1120–1128.
Article
