Clinical Results following Reconstructive Methods in Pelvic Tumor
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea Cancer Center Hospital, Seoul, Korea. dgjeon@kcch.re.kr
- KMID: 2186552
- DOI: http://doi.org/10.4055/jkoa.2007.42.3.298
Abstract
-
PURPOSE: This study evaluated the results of periacetabular resections in patients with pelvic tumors according to the reconstructive methods.
MATERIALS AND METHODS
Twenty-seven patients, who underwent a periacetabular resection with a minimum one year follow up were eligible for this study. There were 20 primary malignant bone tumors, three benign aggressive tumors, three metastatic tumors and one soft tissue sarcoma. According to Enneking's criteria, a type I+II resection was performed in seven patients, type II+III in 17, and type I+II+III in three. The type of reconstructions used were heat treated autogenous bone-THA composite (APC) in 15, a saddle prosthesis in 6, arthrodesis in 2, and a flail hip in 4 patients. The MSTS functional scores and complications according to the type of reconstruction were evaluated.
RESULTS
Eleven (46%) of the 27 patients were in the disease free state and 7 (26%) patients showed local recurrences. Eleven (73%) out of 15 patients with APC and 2 (33%) out of 6 patients with a saddle prosthesis had complications including infections, dislocations and loosening. The final average MSTS score was 19.6 (65%) and all reconstructive methods produced similar functional results.
CONCLUSION
Reconstructions of the acetabulum with a prosthesis after a periacetabular resection had a relatively high rate of complications. A flail hip might be one suitable reconstructive options after a periacetabular resection.
Keyword
MeSH Terms
Figure
-
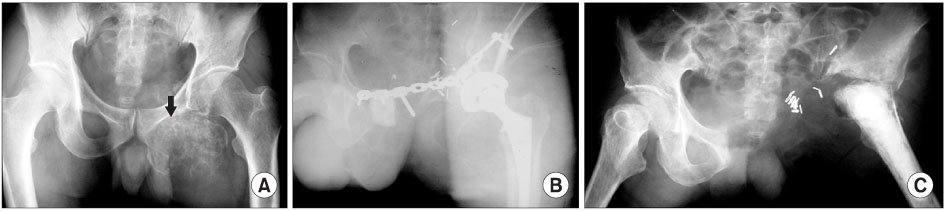
Fig. 1 (A) Plain radiograph shows a huge calcified mass of the pubic ramus extending to the adductor area. (B) A Type II+III resection was performed and reconstructed with heat treated autogenous bone-THA composite. (C) Four months later, all the implants and pasteurized bone were removed and the reconstruction was changed to a flail hip as a result of an infection.
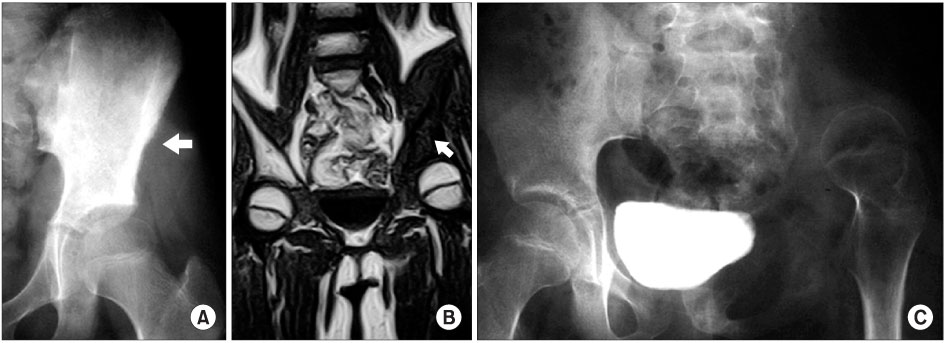
Fig. 2 (A, B) Preoperative radiograph and MRI show a huge calcified mass of the pubis invading the inferior wall of the acetabulum. (C) A Type II+III resection was done and a limited arthrodesis was performed by wiring between the ilium and femoral head.
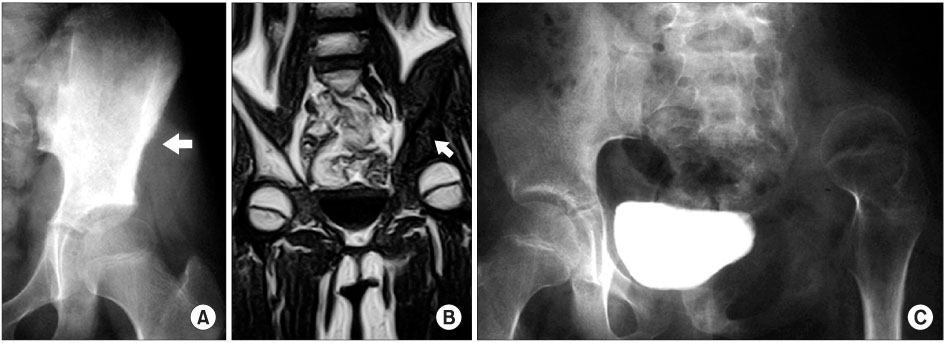
Fig. 3 (A, B) Plain radiograph and MRI show a diffuse lesion involving ilium and acetabulum. (C) Flail hip reconstruction after a type I+II resection was performed and proximal migration of the femoral head is observed.
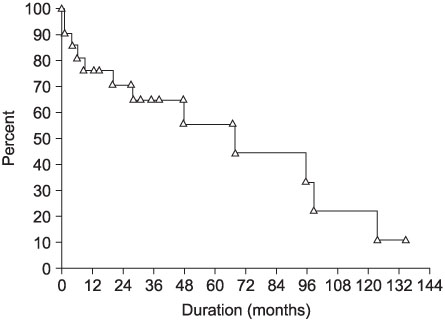
Fig. 4 The Kaplan-Meier survival analysis shows 11% implant survival at 135 months when using heat treated autogenous bone-THA composite or a saddle prosthesis.
Reference
-
1. Aboulafia AJ, Buch R, Mathews J, Li W, Malawer MM. Reconstruction using the saddle prosthesis following excision of primary and metastatic periacetabular tumors. Clin Orthop Relat Res. 1995. 314:203–213.
Article2. Aboulafia AJ, Malawer MM. Surgical management of pelvic and extremity osteosarcoma. Cancer. 1993. 71:Suppl 10. S3358–S3366.
Article3. Bell RS, Davis AM, Wunder JS, Buconjic T, McGoveran B, Gross AE. Allograft reconstruction of the acetabulum after resection of stage-IIB sarcoma. Intermediate-term results. J Bone Joint Surg Am. 1997. 79:1663–1674.4. Capana R, Guernelli N, Ruggieri P. Enneking WF, editor. Periacetabular pelvic resections. Limb salvage in musculoskeletal oncology. 1987. New York: Churchill Livingstone;141–146.5. Enneking WF, Dunham WK. Resection and reconstruction for primary neoplasms involving the innominate bone. J Bone Joint Surg Am. 1978. 60:731–746.
Article6. Enneking WF, Dunham W, Gebhardt MC, Malawer M, Pritchard DJ. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orhop Relat Res. 1993. 286:241–246.
Article7. Enneking WF, Spanier SS, Goodman MA. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop Relat Res. 1980. 153:106–120.
Article8. Harrington KD. The use of hemipelvic allografts or autoclaved grafts for reconstruction after wide resections of malignant tumors of the pelvis. J Bone Joint Surg Am. 1992. 74:331–341.
Article9. Lord CF, Gebhardt MC, Tomford WW, Mankin HJ. Infection in bone allografts. Incidencd, nature and treatment. J Bone Joint Surg Am. 1998. 70:369–376.10. Nieder E, Elson RA, Engelbrecht E, Kasselt MR, Keller A, Steinbrink K. The saddle prosthesis for salvage of the destroyed acetabulum. J Bone Joint Surg Br. 1990. 72:1014–1022.
Article11. O'Connor MI, Sim FH. Salvage of the limb in the treatment of malignant pelvic tumors. J Bone Joint Surg Am. 1989. 71:481–494.12. Pring ME, Weber KL, Unni KK, Sim FH. Chondrosarcoma of the pelvis: a review of sixty-four cases. J Bone Joint Surg Am. 2001. 83:1630–1642.13. Stephenson RB, Kaufer H, Hankin FM. Partial pelvic resection as an alternativ8e to hindquarter amputation for skeletal neoplasms. Clin Orthop Relat Res. 1989. 242:201–211.14. Uchida A, Myoui A, Araki N, Yoshikawa H, Ueda T, Aoki Y. Prosthetic reconstruction for periacetabular malignant tumors. Clin Orthop Relat Res. 1996. 326:238–245.
Article15. Windhager R, Karner J, Kutschera HP, Polterauer P, Salzer-Kuntschik M, Kotz R. Limb salvage in periacetabular sarcomas: review of 21 consecutive cases. Clin Orthop Relat Res. 1996. 331:265–276.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The role of mesh and graft in pelvic reconstructive surgery
- Comparison of Perioperative Complications between Reconstructive Pelvic Surgery and General Gynecologic Surgery
- A Case of Localized fibrous tumor of Pelvic Cavity
- Use of Grafts in Pelvic Reconstructive Surgery
- Prognostic Significance of Renal Pelvic and Medullary Invasion in Renal Cell Carcinoma
