C2 En Bloc Hemilaminectomy and Recapping Using Laminar Screws: A New Approach to Preserve the C2 Extensor Muscles during Intradural Tumor Resection at the C2 Level: A Technical Report
- Affiliations
-
- 1Spine Center and Department of Orthopaedic Surgery, Seoul National University Bundang Hospital, Seongnam, Korea. osdockang@gmail.com
- 2Department of Orthopaedic Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2185309
- DOI: http://doi.org/10.4055/jkoa.2012.47.6.452
Abstract
- Conventional posterior approach for resection of an intradural tumor at C2 involves C2 lamincectomy and detachment of extensor muscles from C2 spinous process. Being major extensors of the cervical spine, the destruction of C2-attached muscles may lead to detrimental consequences, namely, neck pain, limited neck motion, progressive kyphosis, and instability. We report a new technique on exposing and reconstructing the C2 level while preserving C2 extensors for resection of an intradural tumor at C2 level. We performed an en bloc hemilaminectomy of C2 while carefully preserving C2 extensor muscles to adequately expose the dura mater at the C2 level. After removal of the tumor, we proceeded with the reconstruction by recapping the C2 hemilamina using 2 laminar screws.
Figure
-
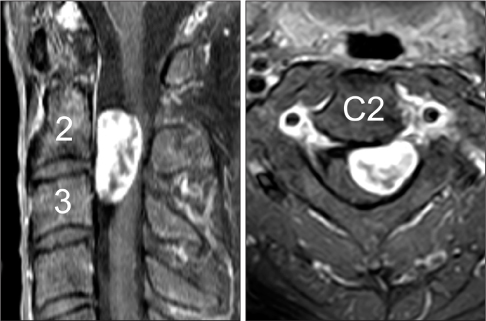
Figure 1 Gadolinium-enhanced magnetic resonance images show an intradural extramedullary mass compressing the spinal cord.

Figure 2 A 3-dimensionally reconstructed image shows the bone procedures done in the current technique. En bloc hemilaminectomy is done with (1) midline splitting of the spinous process and (2) breaking off the lateral gutter of the hemilamina. Muscles attached to C2 remained untouched during the whole procedure. The dura mater is exposed by retracting the left hemilamina to the left side. After tumor resection, the left hemilamina is reattached using 2 laminar screws and 2 miniplates. The laminar screw holes are predrilled prior to hemilaminectomy for accurate bony repositioning and easier screw insertion.
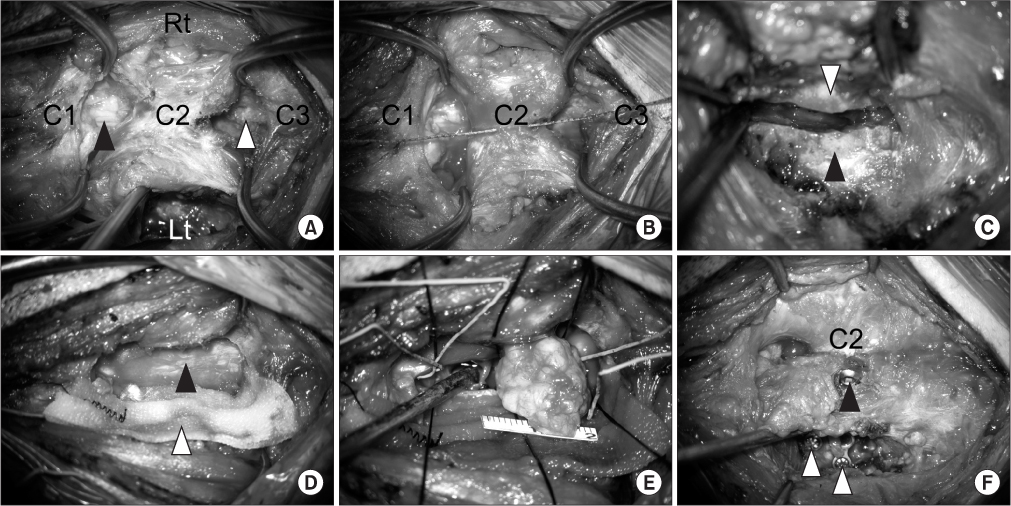
Figure 3 Intraoperative photographs are shown. (A) Midline dissection through the intermuscular planes was done in the areas cranial and caudal to C2. The muscles were retracted laterally using 2 Gelpi retractors. The dura mater was exposed by releasing the ligaments from C1-2 (black arrowhead) and C2-3 (white arrowhead) areas. On the left side, the C2 lamina was exposed between the obliquus capitus and semispinalis. (B) Midline splitting of C2 spinous process was done using a diamond threaded wire. (C) A lateral cut was done between the left lamina (white arrowhead) and the left lateral mass (black arrowhead) using a 1.8 mm burr. (D) The resected left hemilamina was retracted to the left using a Gelpi retractor. It was covered with a large thrombin-soaked cottonoid pledget (white arrowhead) to minimize bleeding (black arrowhead). (E) Intradural tumor mass was removed. (F) The left hemilamina was reattached using 2 laminar screws and 2 minimplates (white arrowheads). Only 1 laminar screw (black arrowhead) is visible on this photograph. Rt, right; Lt, left.
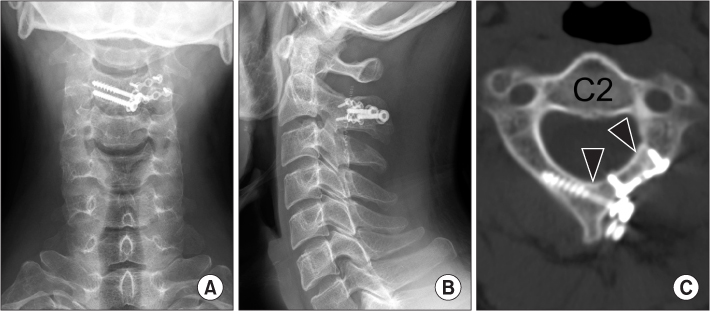
Figure 4 (A, B) Plain radiographs taken at 6 months after the operation show good alignment. (C) A computed tomography scan image taken at 3 months after the operation shows satisfactory union of previously cut surfaces (black arrowheads).
Reference
-
1. De Verdelhan O, Haegelen C, Carsin-Nicol B, et al. MR imaging features of spinal schwannomas and meningiomas. J Neuroradiol. 2005. 32:42–49.
Article2. Okamoto A, Shinomiya K, Furuya K. Reduced neck movement after operations for cervical spondylotic myelopathy. Int Orthop. 1995. 19:295–297.3. Lonstein JE. Post-laminectomy kyphosis. Clin Orthop Relat Res. 1977. (128):93–100.4. Shiraishi T, Yato Y, Yoshida H, Abe T, Ikegami T. New double-door laminoplasty procedures to preserve the muscular attachments to the spinous processes including the axis. Eur J Orthop Surg. 2002. 12:175–180.
Article5. Shiraishi T, Kato M, Yato Y, et al. New techniques for exposure of posterior cervical spine through intermuscular planes and their surgical application. Spine (Phila Pa 1976). 2012. 37:E286–E296.
Article6. Shiraishi T. A new technique for exposure of the cervical spine laminae. Technical note. J Neurosurg. 2002. 96:1 Suppl. 122–126.
Article7. Vasavada AN, Li S, Delp SL. Influence of muscle morphometry and moment arms on the moment-generating capacity of human neck muscles. Spine (Phila Pa 1976). 1998. 23:412–422.
Article8. Abbott R, Feldstein N, Wisoff JH, Epstein FJ. Osteoplastic laminotomy in children. Pediatr Neurosurg. 1992. 18:153–156.
Article9. Kawahara N, Tomita K, Shinya Y, et al. Recapping T-saw laminoplasty for spinal cord tumors. Spine (Phila Pa 1976). 1999. 24:1363–1370.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Atlantoaxial Fixation with a Combination of Pedicle Screws and a Laminar Screw in the Axis for a Unilateral High-riding Vertebral Artery
- Modified Trajectory of C2 Laminar Screw - Double Bicortical Purchase of the Inferiorly Crossing Screw
- Old Atlantoaxial Rotary Subluxation Associated with High-riding Vertebral Arteries: Arthrodesis Using C1 Lateral Mass Screws and C2 Laminar Screws: A Case Report
- Bilateral Pedicle and Crossed Translaminar Screws in C2
- C2 Anatomy for Translaminar Screw Placement Based on Computerized Tomographic Measurements
