J Korean Med Assoc.
2003 Dec;46(12):1117-1127. 10.5124/jkma.2003.46.12.1117.
Diagnostic Approach and Prognostic Factors of Cancers
- Affiliations
-
- 1Department of Pathology, University fo Ulsan College of Medicine, Asan Medical Center, Korea. jaero@amc.seoul.kr, jangsejin@amc.seoul.kr
- KMID: 2183143
- DOI: http://doi.org/10.5124/jkma.2003.46.12.1117
Abstract
- When one follows a systematic approach to make a diagnosis of pathologic of pathologic lesions, it is relatively easy to render a cancer diagnosis in almost all cases in routine daily practice. The first step is to recognize whether or not the specimen contains a lesion and then to determine whether the lesion is neoplastic or nonneoplastic. Since neoplasm is clonal proliferation, neoplastic conditions are usually composed of a single cell type, whereas nonneoplastic conditions consist of multiple different cell types. After a neoplastic condition has been documented, the next step is to decide whether the neoplasm is of an epithelial origin or mesenchymal origin. The main differences between epithelial tumors and mesenchymal tumors include : 1) the tumor cells in epithelial tumors are oval, round to polygonal, while those in mesenchymal tumors are in general spindleshaped : 2) epithelial tumors generally form tumor cell nests, while mesenchymal tumors arrange diffusely without forming tumor cell nests : 3) in epithelial tumors, desmoplastic stroma is wellformed in between tumor cell nests, while in mesenchymal tumors there is no desmoplastic stroma ; and lastly, 4) feeding vessels open in the stroma in epithelial tumors, while they open between tumor cells in mesenchymal tumors. After this one should decide whether the tumor is benign or malignant. The differences between benign and malignant tumors include : 1) differentiation ; 2) growth rate ; 3) growth pattern ; and 4) metastasis. The benign tumor is ell differentiated, grows slowly, shows an expansile growth lattem with encapsulation, and does not metastasize. On the other hand, the malignant tumor is in general poorly differentiated, grows rapidly with frequent mitoses, shows an invasive growth pat-tern without capsular formation, and frequently metastasizes. In general malignant tumors show a high cellularity, tumor necrosis, and nuclear alterations, which include nuclear enlargement with a high nudear/cytoplasmic ratio, hyperchromatism, pleomorphism, prominent nucleolus, and frequent mitoses. The final step is to classify the type of tumor based on the cellular differentiation and gross and microscopic growth patterns based on the light microscopic exarhination of H & E stained slides. For the correct identification of the tumor, immunostaining, electron microscopic evaluation, and molecular diagnostic tools may be required. After establishment of a diagnosis of malignancy, one should think about the prognostic factors. The two wellknown prognostic (factors (category I) applicable in almost all tumors include stage and grade. Therefore, information about the stage and grade should also be included in the pathology report.
Keyword
Figure
-

Figure 1

Figure 2
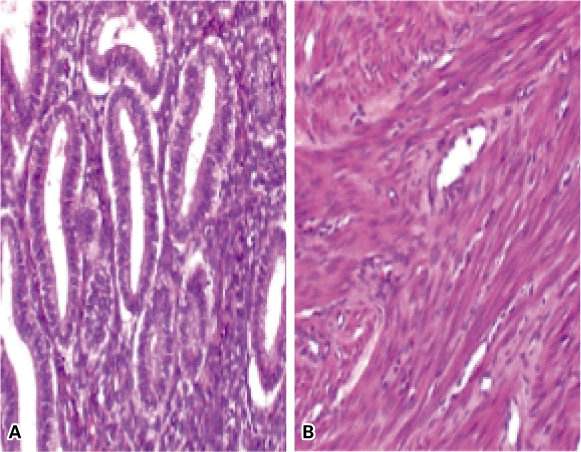
Figure 3

Figure 4

Figure 5
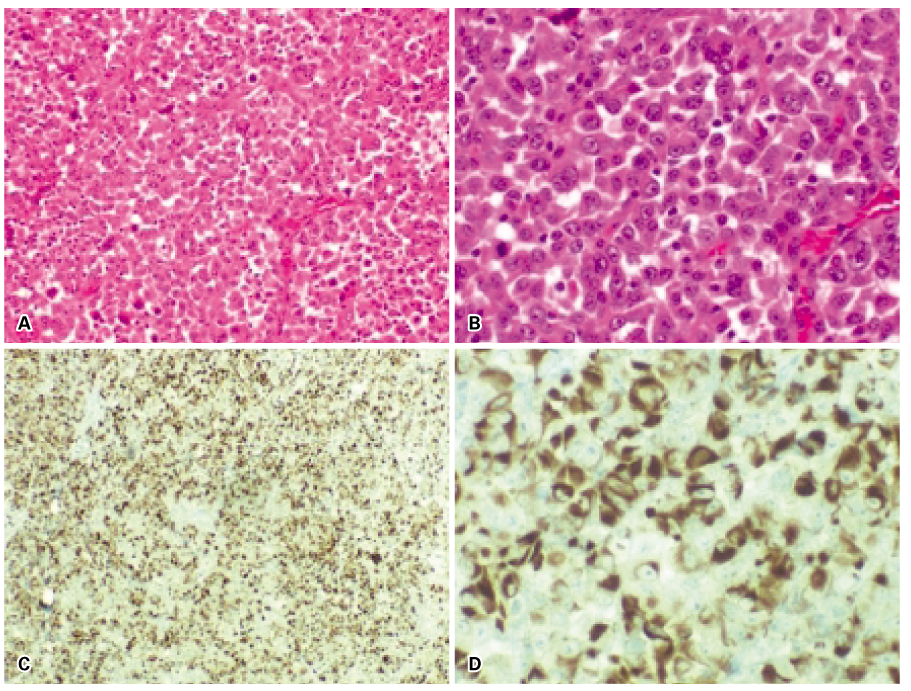
Figure 6

Figure 7
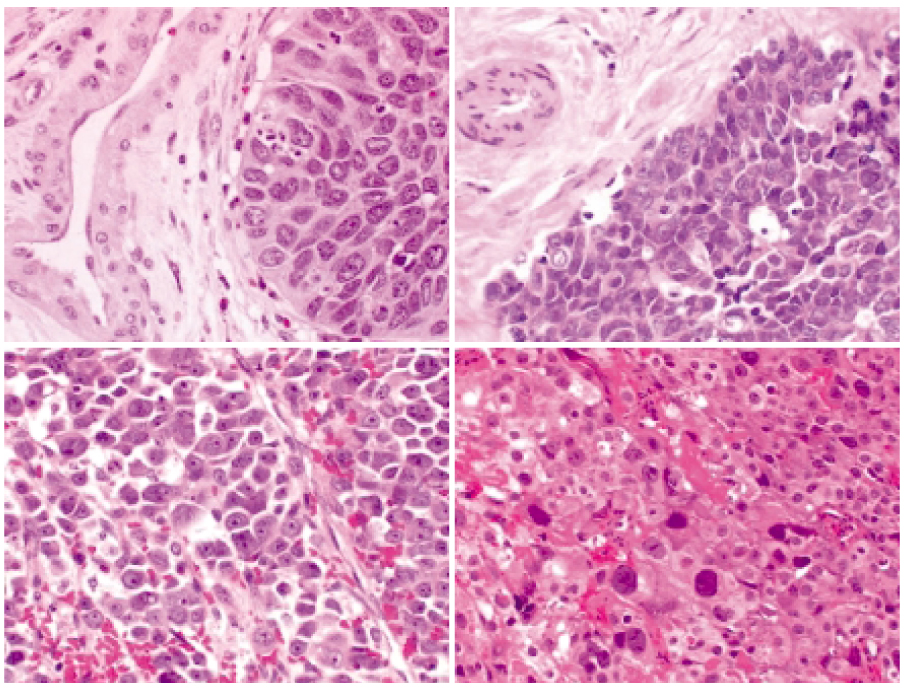
Figure 8

Figure 9
Reference
-
1. Cotran RS, Kumar V, Collins T. Robbins Pathologic Basis of Disease. 1999. 6th ed. Philadelphia: WB Saunders;260–327.2. Lieberman MW, Lebovitz RM. Chapter 24, neoplasia. Anderson's Pathology. 1996. 10th ed. St. Louis: Mosby;513–547.3. Beckwith JB. Wilms' tumor and other renal tumors of childhood : a selective review from the National Wilms' Tumor Study Pathology Center. Hum Pathol. 1983. 14:481–492.
Article4. Fuhrman SA, Lasky LC, Limas C. Prognostic significance of morphologic parameters in renal cell carcinoma. Am J Surg Pathol. 1982. 6:655–663.
Article5. Hammond ME, Fitzgibbons PL, Compton CC, Grignon DJ, Page DL, Pajak TF, et al. Cancer Committee and Conference Participants. College of American Pathologists Conference XXXV: solid tumor prognostic factors-which, how and so what? Summary document and recommendations for implementation. Arch Pathol Lab Med. 2000. 124:958–965.
Article6. Greene FL, Page DL, Fleming ID, Fritz AG, Balch CM, Morrow M, et al. AJCC Cancer Staging Manual. 2002. 6th ed. Springer.7. Giacomarra V, Tirelli G, Papanikolla L, Bussani R. Predictive factors of nodal metastases in oral cavity and oropharynx carcinomas. Laryngoscope. 1999. 109:795–959.
Article8. Jemal A, Murray T, Samuels A, Ghafoor A, Ward E, Thun MJ, et al. Cancer Statistics, 2003. CA. 2003. 53:5–26.
Article9. Black MM, Speer FD. Nuclear grade in cancer tissues. Surg Gynecol Obstet. 1957. 105:97–102.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prognostic Value of TZAP Expression in Various Cancers: TCGA Data Analysis
- Prognostic Factors for Well Differentiated Thyroid Cancer in an Endemic Area
- Epithelial Ovarian Carcinoma: Analysis of Prognostic Factors
- Prognostic factors and Survival in Surgically Resected Superficial Esophageal Cancer
- Adjuvant therapy in cervical cancer patients with high risk factors
