Whole-Body Muscle MRI in Patients with Hyperkalemic Periodic Paralysis Carrying the SCN4A Mutation T704M: Evidence for Chronic Progressive Myopathy with Selective Muscle Involvement
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Medical Convergence Research Institute, Severance Biomedical Science Institute, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Neurology, Yonsei University College of Medicine, Seoul, Korea. hayshin@yuhs.ac
- 3Department of Neurology, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2179752
- DOI: http://doi.org/10.3988/jcn.2015.11.4.331
Abstract
- BACKGROUND AND PURPOSE
Hyperkalemic periodic paralysis (hyperKPP) is a muscle sodium-ion channelopathy characterized by recurrent paralytic attacks. A proportion of affected individuals develop fixed or chronic progressive weakness that results in significant disability. However, little is known about the pathology of hyperKPP-induced fixed weakness, including the pattern of muscle involvement. The aim of this study was to characterize the patterns of muscle involvement in hyperKPP by whole-body magnetic resonance imaging (MRI).
METHODS
We performed whole-body muscle MRI in seven hyperKPP patients carrying the T704M mutation in the SCN4A skeletal sodium-channel gene. Muscle fat infiltration, suggestive of chronic progressive myopathy, was analyzed qualitatively using a grading system and was quantified by the two-point Dixon technique.
RESULTS
Whole-body muscle MRI analysis revealed muscle atrophy and fatty infiltration in hyperKPP patients, especially in older individuals. Muscle involvement followed a selective pattern, primarily affecting the posterior compartment of the lower leg and anterior thigh muscles. The muscle fat fraction increased with patient age in the anterior thigh (r=0.669, p=0.009), in the deep posterior compartment of the lower leg (r=0.617, p=0.019), and in the superficial posterior compartment of the lower leg (r=0.777, p=0.001).
CONCLUSIONS
Our whole-body muscle MRI findings provide evidence for chronic progressive myopathy in hyperKPP patients. The reported data suggest that a selective pattern of muscle involvement-affecting the posterior compartment of the lower leg and the anterior thigh-is characteristic of chronic progressive myopathy in hyperKPP.
Keyword
MeSH Terms
Figure
-
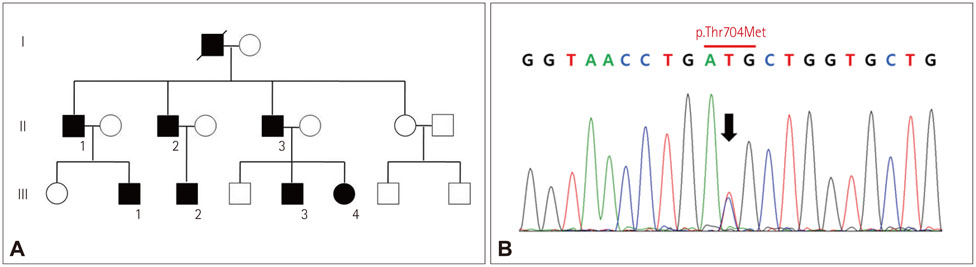
Fig. 1 Pedigree of a family with hyperkalemic periodic paralysis and mutation of the SCN4A gene. A: Family pedigree with affected individuals shown as solid symbols. B: Genomic DNA sequence electropherogram of patient II:1 showing a heterozygous p.T704M SCN4A mutation arrow, which is present in all patients, but not in healthy family members.
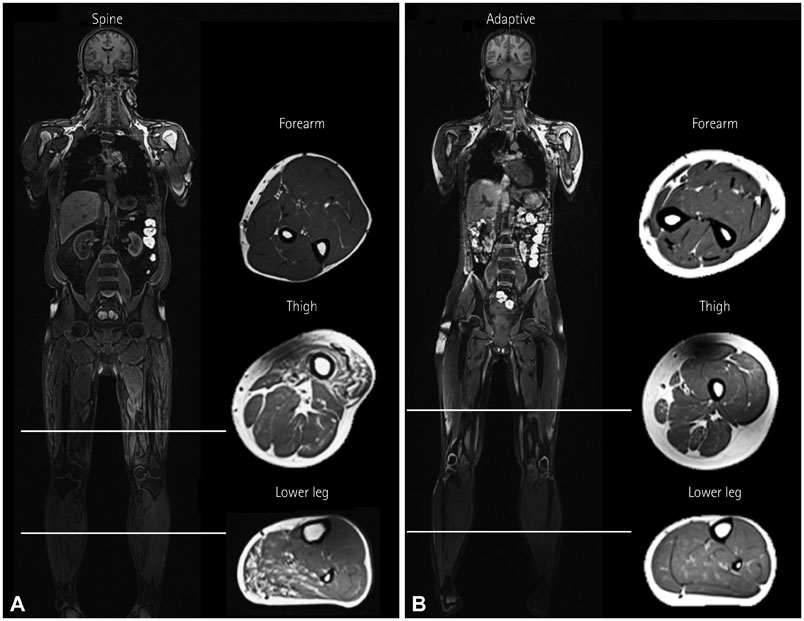
Fig. 2 Whole-body MRI (T1-weighted images) of patients II:1 (A) and III:4 (B). A: Muscle atrophy with fatty infiltration is demonstrated in the anterior compartment of the thigh and the posterior compartment of the lower leg in patient II:1, the oldest (49-year-old) patient in this study. B: Conversely, in patient III:4, the youngest (14-year-old) patient in this study, all muscles appear normal.
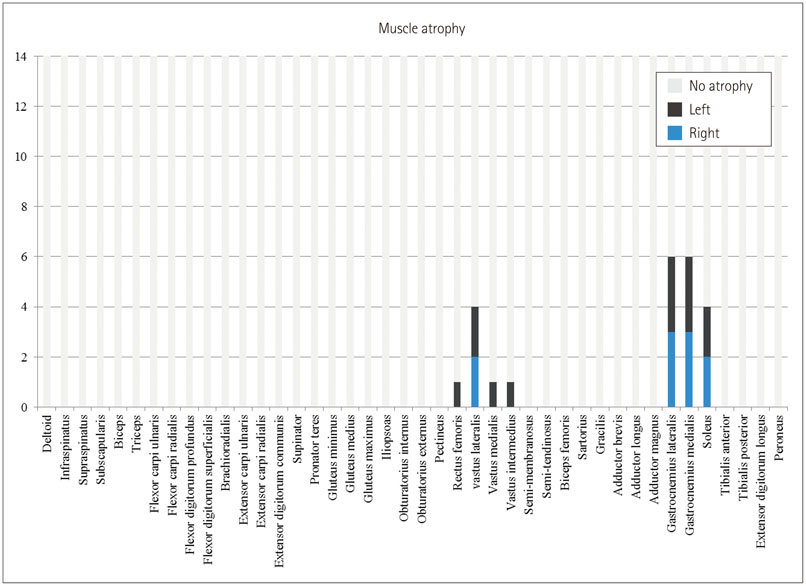
Fig. 3 Frequency of muscle atrophy observed in different muscle groups. All atrophic muscles are in the posterior compartment of the lower leg or the anterior compartment of thigh.
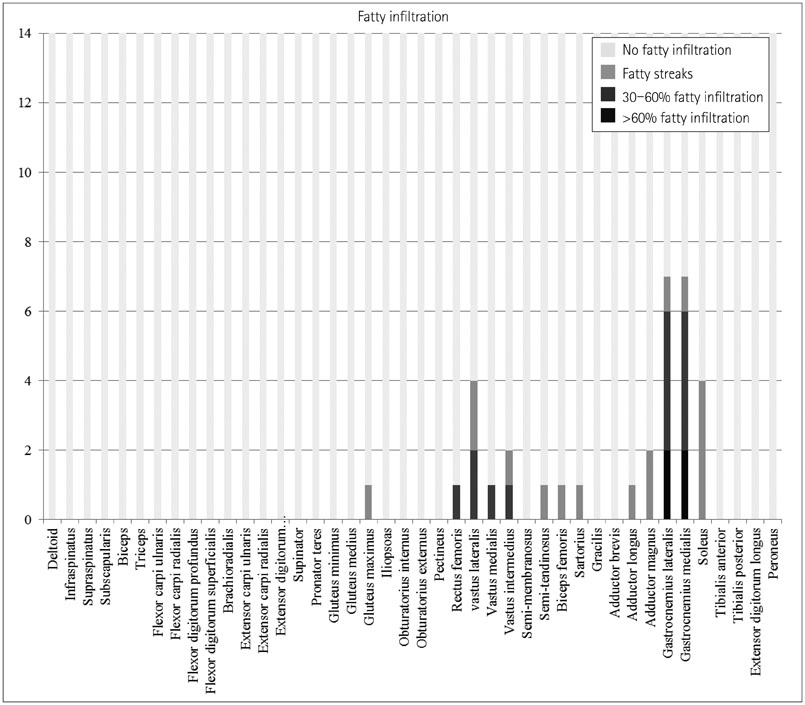
Fig. 4 Frequency and severity of fatty infiltration in different muscle groups. All fatty infiltrated muscles are in the lower extremities, with the muscles in the posterior compartment of lower leg more frequently and severely affected than those in other parts of the lower extremities.
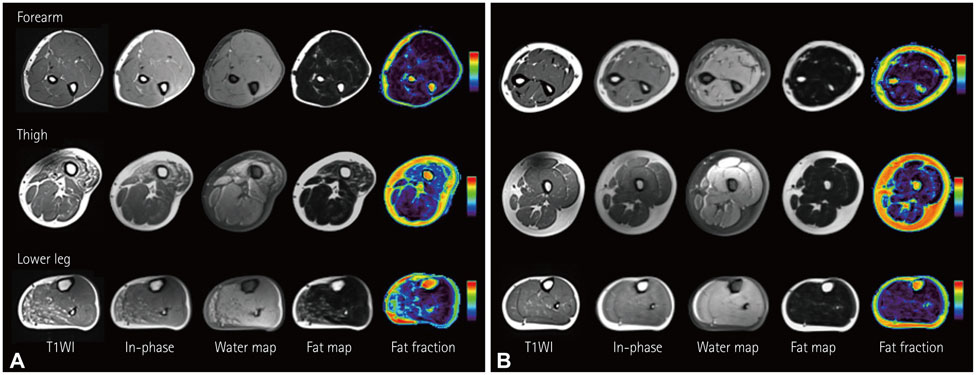
Fig. 5 Muscle fat quantification of patient II:1 (A) and III:4 (B). A: Increased muscle fat fraction with muscle atrophy is demonstrated in the anterior thigh and posterior compartment of the lower leg in patient II:1, the oldest (49-year-old) patient in this study. B: Conversely, in patient III:4, the youngest (14-year-old) patient in this study, the muscles of forearm, thigh, and lower leg do not show fatty infiltration or muscle atrophy.

Fig. 6 Two-point Dixon measurement of muscle fat fraction plotted against patient age. We observe that muscle fat fraction increases with age in the superficial posterior compartment of the lower leg (r=0.777; p=0.001).
Reference
-
1. Lee SC, Kim HS, Park YE, Choi YC, Park KH, Kim DS. Clinical diversity of SCN4A-mutation-associated skeletal muscle sodium channelopathy. J Clin Neurol. 2009; 5:186–191.
Article2. Ptácek LJ, George AL Jr, Griggs RC, Tawil R, Kallen RG, Barchi RL, et al. Identification of a mutation in the gene causing hyperkalemic periodic paralysis. Cell. 1991; 67:1021–1027.
Article3. Bradley WG, Taylor R, Rice DR, Hausmanowa-Petruzewicz I, Adelman LS, Jenkison M, et al. Progressive myopathy in hyperkalemic periodic paralysis. Arch Neurol. 1990; 47:1013–1017.
Article4. Charles G, Zheng C, Lehmann-Horn F, Jurkat-Rott K, Levitt J. Characterization of hyperkalemic periodic paralysis: a survey of genetically diagnosed individuals. J Neurol. 2013; 260:2606–2613.
Article5. Miller TM, Dias da Silva MR, Miller HA, Kwiecinski H, Mendell JR, Tawil R, et al. Correlating phenotype and genotype in the periodic paralyses. Neurology. 2004; 63:1647–1655.
Article6. Amarteifio E, Nagel AM, Weber MA, Jurkat-Rott K, Lehmann-Horn F. Hyperkalemic periodic paralysis and permanent weakness: 3-T MR imaging depicts intracellular 23Na overload--initial results. Radiology. 2012; 264:154–163.
Article7. Hollingsworth KG, de Sousa PL, Straub V, Carlier PG. Towards harmonization of protocols for MRI outcome measures in skeletal muscle studies: consensus recommendations from two TREAT-NMD NMR workshops, 2 May 2010, Stockholm, Sweden, 1-2 October 2009, Paris, France. Neuromuscul Disord. 2012; 22:Suppl 2. S54–S67.
Article8. Theodorou DJ, Theodorou SJ, Kakitsubata Y. Skeletal muscle disease: patterns of MRI appearances. Br J Radiol. 2012; 85:e1298–e1308.
Article9. Mendell JR, Florence J. Manual muscle testing. Muscle Nerve. 1990; 13:Suppl. S16–S20.
Article10. Mercuri E, Pichiecchio A, Counsell S, Allsop J, Cini C, Jungbluth H, et al. A short protocol for muscle MRI in children with muscular dystrophies. Eur J Paediatr Neurol. 2002; 6:305–307.
Article11. Quijano-Roy S, Avila-Smirnow D, Carlier RY. WB-MRI muscle study group. Whole body muscle MRI protocol: pattern recognition in early onset NM disorders. Neuromuscul Disord. 2012; 22:Suppl 2. S68–S84.
Article12. Park HJ, Hong JM, Suh GI, Shin HY, Kim SM, Sunwoo IN, et al. Heterogeneous characteristics of Korean patients with dysferlinopathy. J Korean Med Sci. 2012; 27:423–429.
Article13. Takahashi T, Aoki M, Tateyama M, Kondo E, Mizuno T, Onodera Y, et al. Dysferlin mutations in Japanese Miyoshi myopathy: relationship to phenotype. Neurology. 2003; 60:1799–1804.
Article14. Wren TA, Bluml S, Tseng-Ong L, Gilsanz V. Three-point technique of fat quantification of muscle tissue as a marker of disease progression in Duchenne muscular dystrophy: preliminary study. AJR Am J Roentgenol. 2008; 190:W8–W12.
Article15. Ma J. Dixon techniques for water and fat imaging. J Magn Reson Imaging. 2008; 28:543–558.
Article16. Smith AC, Parrish TB, Abbott R, Hoggarth MA, Mendoza K, Chen YF, et al. Muscle-fat MRI: 1.5 Tesla and 3.0 Tesla versus histology. Muscle Nerve. 2014; 50:170–176.
Article17. Noble JJ, Keevil SF, Totman J, Charles-Edwards GD. In vitro and in vivo comparison of two-, three- and four-point Dixon techniques for clinical intramuscular fat quantification at 3 T. Br J Radiol. 2014; 87:20130761.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Familial hyperkalemic periodic paralysis caused by a de novo mutation in the sodium channel gene SCN4A
- Electrophysiological Changes by Exercise and Cold Provocation Test in a Patient with Hyperkalemic Periodic Paralysis
- A Case of Hyperkalemic Periodic Paralysis Induced by Diabetic Nephropathy
- Clinical Diversity of SCN4A-Mutation-Associated Skeletal Muscle Sodium Channelopathy
- An atypical phenotype of hypokalemic periodic paralysis caused by a mutation in the sodium channel gene SCN4A
