Progression Rate of Aortic Valve Stenosis in Korean Patients
- Affiliations
-
- 1Division of Cardiology, Cardiovascular Imaging Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. parksmc@gmail.com
- KMID: 2177313
- DOI: http://doi.org/10.4250/jcu.2010.18.4.127
Abstract
- BACKGROUND
Although there were studies about ethnic differences in aortic valve thickness and calcification that they may play a role in aortic valvular stenosis (AVS) progression, few studies about the progression rate of AVS in Asian population have been reported. The purpose of this study was to evaluate the progression rate of AVS in Korean patients.
METHODS
We retrospectively analyzed 325 patients (181 men, age: 67 +/- 13 years) with AVS who had 2 or more echocardiograms at least 6 months apart from 2003 to 2008. The patients with other significant valvular diseases or history of cardiac surgery were excluded. The progression rate of AVS was expressed in terms of increase in maximum aortic jet velocity per year (meter/second/year).
RESULTS
Baseline AVS was mild in 207 (64%), moderate in 81 (25%), and severe in 37 (11%). There were no significant differences among the three groups in terms of age, gender, hypertension, smoking, and hypercholesterolemia. The mean progression rate was 0.12 +/- 0.23 m/s/yr and more rapid in severe AVS (0.28 +/- 0.36 m/s/yr) when compared to moderate (0.14 +/- 0.26 m/s/yr) and mild AVS (0.09 +/- 0.18 m/s/yr) (p < 0.001). The progression rate in bicuspid AVS was significantly higher than other AVS (0.23 +/- 0.35 vs. 0.11 +/- 0.20 m/s/yr, p = 0.002). By multivariate analysis, initial maximum aortic jet velocity (Beta = 0.175, p = 0.003), bicuspid aortic valve (Beta = 0.127, p = 0.029), and E velocity (Beta = -0.134, p = 0.018) were significantly associated with AVS progression.
CONCLUSION
The progression rate of AVS in Korean patients is slower than that reported in Western population. Therefore, ethnic difference should be considered for the follow-up of the patients with AVS.
MeSH Terms
-
Aortic Valve
Aortic Valve Stenosis
Asian Continental Ancestry Group
Bicuspid
Constriction, Pathologic
Disease Progression
Follow-Up Studies
Heart Valve Diseases
Humans
Hypercholesterolemia
Hypertension
Male
Multivariate Analysis
Natural History
Retrospective Studies
Smoke
Smoking
Thoracic Surgery
Aortic Valve
Heart Valve Diseases
Smoke
Figure
-
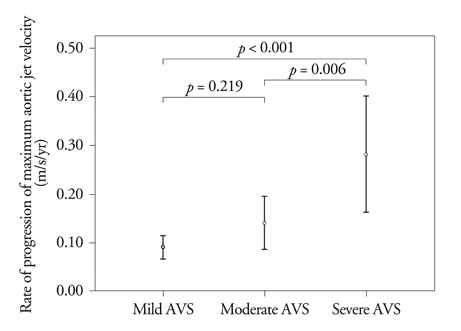
Fig. 1 Progression rate of maximum aortic jet velocity according to AVS severity. Bars, mean ± SD. A p value indicates difference between groups based on scheffe's multiple comparison test. AVS: aortic valvular stenosis.
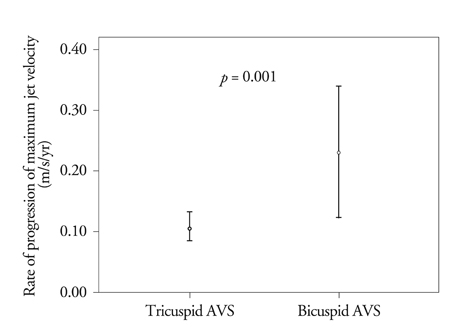
Fig. 2 Progression rate of maximum aortic jet velocity with and without bicuspid aortic valve. Bars, mean ± SD. AVS: aortic valvular stenosis.
Cited by 2 articles
-
Statins Have No Role in Preventing the Progression of Aortic Valve Sclerosis
Jeong-Hun Seo, Kwang-Jin Chun, Bong-Ki Lee, Byung-Ryul Cho, Dong Ryeol Ryu
J Cardiovasc Imaging. 2018;26(4):229-237. doi: 10.4250/jcvi.2018.26.e27.Early Aortic Valve Replacement in Symptomatic Normal-Flow, Low-Gradient Severe Aortic Stenosis: A Propensity Score–Matched Retrospective Cohort Study
Kyu Kim, Iksung Cho, Kyu-Yong Ko, Seung-Hyun Lee, Sak Lee, Geu-Ru Hong, Jong-Won Ha, Chi Young Shim
Korean Circ J. 2023;53(11):744-755. doi: 10.4070/kcj.2023.0022.
Reference
-
1. Otto CM, Burwash IG, Legget ME, Munt BI, Fujioka M, Healy NL, Kraft CD, Miyake-Hull CY, Schwaegler RG. Prospective study of asymptomatic valvular aortic stenosis. Clinical, echocardiographic, and exercise predictors of outcome. Circulation. 1997. 95:2262–2270.
Article2. Otto CM, Pearlman AS, Gardner CL. Hemodynamic progression of aortic stenosis in adults assessed by Doppler echocardiography. J Am Coll Cardiol. 1989. 13:545–550.
Article3. Rosenhek R, Binder T, Porenta G, Lang I, Christ G, Schemper M, Maurer G, Baumgartner H. Predictors of outcome in severe, asymptomatic aortic stenosis. N Engl J Med. 2000. 343:611–617.
Article4. Rosenhek R, Klaar U, Schemper M, Scholten C, Heger M, Gabriel H, Binder T, Maurer G, Baumgartner H. Mild and moderate aortic stenosis. Natural history and risk stratification by echocardiography. Eur Heart J. 2004. 25:199–205.
Article5. Bahler RC, Desser DR, Finkelhor RS, Brener SJ, Youssefi M. Factors leading to progression of valvular aortic stenosis. Am J Cardiol. 1999. 84:1044–1048.
Article6. Peter M, Hoffmann A, Parker C, Lüscher T, Burckhardt D. Progression of aortic stenosis. Role of age and concomitant coronary artery disease. Chest. 1993. 103:1715–1719.
Article7. Sashida Y, Rodriguez CJ, Boden-Albala B, Jin Z, Elkind MS, Liu R, Rundek T, Sacco RL, DiTullio MR, Homma S. Ethnic differences in aortic valve thickness and related clinical factors. Am Heart J. 2010. 159:698–704.
Article8. Nasir K, Katz R, Takasu J, Shavelle DM, Detrano R, Lima JA, Blumenthal RS, O'Brien K, Budoff MJ. Ethnic differences between extra-coronary measures on cardiac computed tomography: multi-ethnic study of atherosclerosis (MESA). Atherosclerosis. 2008. 198:104–114.
Article9. Sim DS, Park JC, Kim W, Kim JH, Park WS, Park OY, Ahn YK, Jeong MH, Cho JG, Oh BS, Ahn BH, Kim SH, Kang JC. Prognostic factors for medically treated patients with valvular aortic stenosis. Chonnam Med J. 2003. 39:29–36.10. Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, Iung B, Otto CM, Pellikka PA, Quiñones M. American Society of Echocardiography. European Association of Echocardiography. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr. 2009. 22:1–23. quiz 101-2.
Article11. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, Reichek N. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986. 57:450–458.
Article12. Oh JK, Taliercio CP, Holmes DR Jr, Reeder GS, Bailey KR, Seward JB, Tajik AJ. Prediction of the severity of aortic stenosis by Doppler aortic valve area determination: prospective Doppler-catheterization correlation in 100 patients. J Am Coll Cardiol. 1988. 11:1227–1234.
Article13. Kume T, Kawamoto T, Okura H, Watanabe N, Toyota E, Neishi Y, Okahashi N, Yamada R, Yoshida K. Rapid progression of mild to moderate aortic stenosis in patients older than 80 years. J Am Soc Echocardiogr. 2007. 20:1243–1246.
Article14. Palta S, Pai AM, Gill KS, Pai RG. New insights into the progression of aortic stenosis: implications for secondary prevention. Circulation. 2000. 101:2497–2502.
Article15. Edwards JE. The congenital bicuspid aortic valve. Circulation. 1961. 23:485–488.16. Villari B, Hess OM, Kaufmann P, Krogmann ON, Grimm J, Krayenbuehl HP. Effect of aortic valve stenosis (pressure overload) and regurgitation (volume overload) on left ventricular systolic and diastolic function. Am J Cardiol. 1992. 69:927–934.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Expanding transcatheter aortic valve replacement into uncharted indications
- Unicommisural Unicuspid Aortic Valve with Very Severe Aortic Stenosis in a 17-Year-Old Female
- Percutaneous transluminal balloon valvuloplasty for congenital pulmonary valve stenosis and aortic valve stenosis
- Multimodality Imaging for the Assessment of Severe Aortic Stenosis
- A Case of Severe Aortic Stenosis Patient With High Operative Risk Treated by Transcatheter Aortic-Valve Implantation
