Chonnam Med J.
2011 Apr;47(1):39-42. 10.4068/cmj.2011.47.1.39.
Penile Growth in Response to Human Chorionic Gonadotropin (hCG) Treatment in Patients with Idiopathic Hypogonadotrophic Hypogonadism
- Affiliations
-
- 1Department of Urology, Chonnam National University Medical School, Sexual Medicine Research Center, Chonnam National University, Gwangju, Korea. uropark@gmail.com
- KMID: 2172243
- DOI: http://doi.org/10.4068/cmj.2011.47.1.39
Abstract
- Penile growth is under androgenic control. Human chorionic gonadotropin (hCG) has a stimulatory effect on testicular steroidogenesis and penile growth. The purpose of this study was to evaluate the effect of hCG treatment on the gonadal response and penile growth in male idiopathic hypogonadotrophic hypogonadism (IHH) presenting with micropenis. A total of 20 IHH patients who met the criteria for micropenis were included in this study. hCG (1,500-2,000 IU) was administrated intramuscularly, 3 times per week, for 8 weeks. Basic laboratory and hormonal indexes (including serum testosterone and LH levels), penis length (flaccid and stretched), and testicular volume were measured before and 24 weeks after hCG treatment. The patients' mean age was 18.9 years (range, 12 to 24 years). The mean serum testosterone level was significantly increased after hCG treatment (baseline, 2, 4, 12, and 24 weeks: 0.90+/-1.35 ng/ml, 1.77+/-1.31 ng/ml, 3.74+/-2.24 ng/ml, 5.49+/-1.70 ng/ml, and 5.58+/-1.75 ng/ml, respectively; p<0.05). Mean penile length also increased significantly 24 weeks after treatment (flaccid length: from 3.39+/-1.03 cm to 5.14+/-1.39 cm; stretched length: from 5.41+/-1.43 cm to 7.45+/-1.70 cm; p<0.001). Mean testicular volumes increased significantly as well (left: from 5.45 cc to 6.83 cc; right: from 5.53 cc to 7.03 cc). There were no remarkable adverse effects of the hCG treatment. The hCG treatment increased the serum testosterone level, penile length, and testicular volume in IHH patients. Our results suggest that hCG treatment has a beneficial effect on gonadal function and penile growth in patients with IHH presenting with micropenis.
MeSH Terms
Figure
-
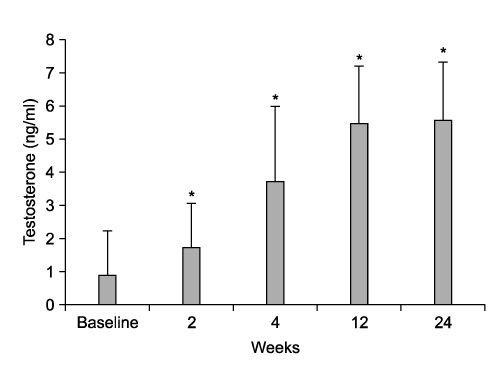
FIG. 1 Change in the mean serum testosterone level after hCG treatment. *: p<0.05 vs baseline.
Reference
-
1. Kallmann FJ, Schoenfeld WA, Barrera SE. The genetic aspects of primary eunuchoidism. Am J Ment Defic. 1994. 48:203–236.2. Kirk JM, Savage MO, Grant DB, Bouloux PM, Besser GM. Gonadal function and response to human chorionic and menopausal gonadotrophin therapy in male patients with idiopathic hypogonadotrophic hypogonadism. Clin Endocrinol (Oxf). 1994. 41:57–63.
Article3. Bistritzer T, Lunenfeld B, Passwell JH, Theodor R. Hormonal therapy and pubertal development in boys with selective hypogonadotropic hypogonadism. Fertil Steril. 1989. 52:302–306.
Article4. Lee PA, Mazur T, Danish R, Amrhein J, Blizzard RM, Money J, et al. Micropenis. I. Criteria, etiologies and classification. Johns Hopkins Med J. 1980. 146:156–163.5. Yoshimoto Y, Moridera K, Imura H. Restoration of normal pituitary gonadotropin reserve by administration of luteinizing-hormone-releasing hormone in patients with hypogonadotropic hypogonadism. N Engl J Med. 1975. 292:242–245.
Article6. Hoffman AR, Crowley WF Jr. Induction of puberty in men by long-term pulsatile administration of low-dose gonadotropin-releasing hormone. N Engl J Med. 1982. 307:1237–1241.
Article7. Reitano JF, Caminos-Torres R, Snyder PJ. Serum LH and FSH responses to the repetitive administration of gonadotropin-releasing hormone in patients with idiopathic hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 1975. 41:1035–1042.
Article8. Snyder PJ, Rudenstein RS, Gardner DF, Rothman JG. Repetitive infusion of gonadotropin-releasing hormone distinguishes hypothalamic from pituitary hypogonadism. J Clin Endocrinol Metab. 1979. 48:864–868.
Article9. Menon PS, Khatwa UA. The child with micropenis. Indian J Pediatr. 2000. 67:455–460.
Article10. Bistritzer T, Lunenfeld B, Passwell JH, Theodor R. Hormonal therapy and pubertal development in boys with selective hypogonadotropic hypogonadism. Fertil Steril. 1989. 52:302–306.
Article11. Schopohl J, Mehltretter G, von Zumbusch R, Eversmann T, von Werder K. Comparison of gonadotropin-releasing hormone and gonadotropin therapy in male patients with idiopathic hypothalamic hypogonadism. Fertil Steril. 1991. 56:1143–1150.
Article12. Burris AS, Rodbard HW, Winters SJ, Sherins RJ. Gonadotropin therapy in men with isolated hypogonadotropic hypogonadism: the response to human chorionic gonadotropin is predicted by initial testicular size. J Clin Endocrinol Metab. 1988. 66:1144–1151.
Article13. Ley SB, Leonard JM. Male hypogonadotropic hypogonadism: factors influencing response to human chorionic gonadotropin and human menopausal gonadotropin, including prior exogenous androgens. J Clin Endocrinol Metab. 1985. 61:746–752.
Article14. Van Wagenen G, Simpson ME. Embryology of the ovary and testis, Homo sapiens and Macaca mulatta. 1965. New Haven: Yale University Press.15. Zachmann M, Prader A, Kind HP, Häfliger H, Budliger H. Testicular volume during adolescence. Cross-sectional and longitudinal studies. Helv Paediatr Acta. 1974. 29:61–72.16. Waaler PE, Thorsen T, Stoa KF, Aarskog D. Studies in normal male puberty. Acta Paediatr Scand Suppl. 1974. 249:1–36.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Investigation of Male Hypogonadism
- Effect of treatment in men with idiopathic hypogonadotropichypodonadism
- Induction of Fertility in a Man with Acquired Hypogonadotropic Hypogonadism
- Morphometric and ultrastructural studies on the effects of human chorionic gonadotropin (hCG) in mouse uterus.
- Therapy with Human Chorionic Gonadotropin and Human Menopausal Gonadotropin in Men with Hypogonadotropic Hypogonadism
