Ann Dermatol.
2011 Feb;23(1):95-97. 10.5021/ad.2011.23.1.95.
Unilateral Nevoid Acanthosis Nigricans with a Submammary Location
- Affiliations
-
- 1Department of Dermatology, School of Medicine and Medical Research Institute, Chungbuk National University, Cheongju, Korea. jyl@chungbuk.ac.kr
- KMID: 2171963
- DOI: http://doi.org/10.5021/ad.2011.23.1.95
Abstract
- Unilateral nevoid acanthosis nigricans (AN) is an exceedingly rare form of AN, which is a benign disorder of keratinization. The lesions of unilateral nevoid AN are distributed unilaterally while the histopathologic findings are similar to the common form of AN, and this is characterized by hyperkeratosis, papillomatosis and moderate acanthosis. A 19-year-old female presented with asymptomatic brownish pigmented plaques on the medial side of the left submammary area. Based on her clinical and histopathologic findings, a diagnosis of unilateral nevoid AN was made. She was treated with topical tretinoin and her skin lesions were almost cleared 9 months after her first visit to our clinic. Various previous reports have described the localization of this disorder, but there has been no previous case report with the clinical manifestations on the unilateral submammary area. Therefore, we herein report the first case of unilateral nevoid AN with an unusual submammary location.
Keyword
MeSH Terms
Figure
-
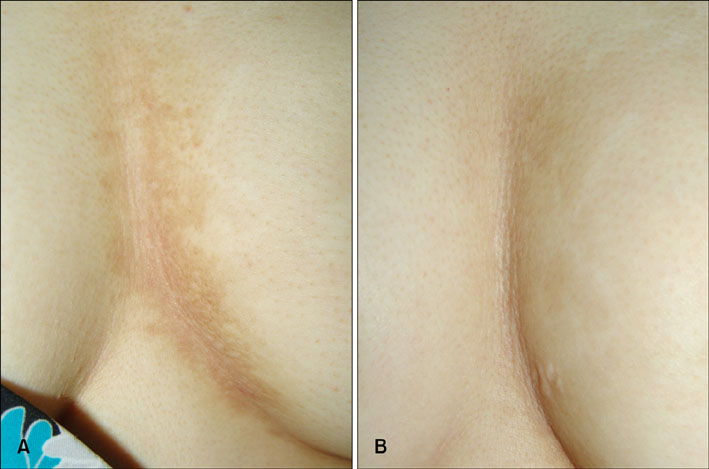
Fig. 1 (A) Linear verrucous brownish plaques on the intermammary to left submammary area and (B) substantial clearance 9 months after the initiation of topical tretinoin treatment.

Fig. 2 (A) Hyperkeratosis, papillomatosis and moderate acanthosis are seen in the epidermis (H&E, ×100). All the immunoreactivities for estrogen receptor (B), progesterone receptor (C) and androgen receptor (D) are negative in the epidermis (immunoperoxidase, ×400). (B) Inset: immunohistochemistry for estrogen receptor in the ductal carcinoma cells of the breast as the positive control (immunoperoxidase, ×400).
Reference
-
1. Schwartz RA. Acanthosis nigricans. J Am Acad Dermatol. 1994. 31:1–19.
Article2. Ersoy-Evans S, Sahin S, Mancini AJ, Paller AS, Guitart J. The acanthosis nigricans form of epidermal nevus. J Am Acad Dermatol. 2006. 55:696–698.
Article3. Curth HO. Unilateral epidermal naevus resembling acanthosis nigricans. Br J Dermatol. 1976. 95:433–436.
Article4. Kim MY, Lee JS, Kim HO, Park YM. A case of nevoid acanthosis nigricans. Acta Derm Venereol. 2004. 84:234–235.
Article5. Lee JH, Kim MY, Kim HO, Park YM. Nevoid acanthosis nigricans localized to the umbilicus: successful treatment with topical tretinoin. Ann Dermatol. 2005. 17:24–26.
Article6. Krishnaram AS. Unilateral nevoid acanthosis nigricans. Int J Dermatol. 1991. 30:452–453.
Article7. Kim SK, Kim YC. Nevoid acanthosis nigricans localized to the umbilicus. J Dermatol. 2006. 33:433–434.
Article8. Lee KH, Park HJ, Lee JY, Cho BK. A case of unilateral acanthosis nigricans. Korean J Dermatol. 2002. 40:1276–1278.9. Cruz PD Jr, Hud JA Jr. Excess insulin binding to insulin-like growth factor receptors: proposed mechanism for acanthosis nigricans. J Invest Dermatol. 1992. 98:82S–85S.
Article10. Person JR, Longcope C. Becker's nevus: an androgen-mediated hyperplasia with increased androgen receptors. J Am Acad Dermatol. 1984. 10:235–238.
Article11. Darmstadt GL, Yokel BK, Horn TD. Treatment of acanthosis nigricans with tretinoin. Arch Dermatol. 1991. 127:1139–1140.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Unilateral Nevoid Telangiectasia Associated With Acanthosis Nigricans
- A Case of Unilateral Acanthosis Nigricans
- Unilateral Acanthosis Nigricans on Non-flexural Area
- Nevoid Acanthosis Nigricans Localized to the Umbilicus: Successful Treatment with Topical Tretinoin
- Acanthosis Nigricans Associated with Vitiligo
