Composite Tumor Associating Trichoblastoma and Seborrheic Keratosis
- Affiliations
-
- 1Department of Dermatology, Kyung Hee University College of Medicine, Seoul, Korea. bellotte@hanmail.net
- KMID: 2171461
- DOI: http://doi.org/10.5021/ad.2015.27.5.601
Abstract
- Seborrheic keratosis is a common benign epidermal tumor histologically composed of basaloid and squamous cells. It mainly occurs on the face, scalp, and trunk, and presents clinically as a well-circumscribed, brownish to black papule, nodule, or plaque. Trichoblastoma is a relatively rare benign, slow-growing tumor showing differentiation toward the primitive hair follicle. It clinically manifests as a solitary, skin to erythematous colored, well-circumscribed dermal nodule located predominantly on the head and neck with a predilection for the scalp. Histologically, a well-demarcated mass of follicular germinative cells that show various degrees of differentiation, arranged in lobules, sheets, and nests, is located in the dermis or subcutaneous fat layer. We report the case of a 28-year-old female patient with a solitary, 2.0x4.0-cm black plaque with a 0.7-cm skin-colored nodule on the scalp. Histologically, the entire black plaque had prominent hyperkeratosis, acanthosis, and papillomatosis with horn cysts. The central nodule showed well-circumscribed, various-sized dermal tumor lobules without a connection to the overlying epidermis. The lobular aggregation was composed of numerous basaloid epithelial nests and multiple primitive papillary structures with distinct peripheral palisading of nuclei. According to these findings, the scalp lesion was diagnosed as a composite tumor associating trichoblastoma and seborrheic keratosis.
MeSH Terms
Figure
-

Fig. 1 A 2.0×4.0-cm dark pigmented, verrucous plaque on the scalp. Centrally, a distinct 0.7-cm skin-colored, hairless nodule was observed.
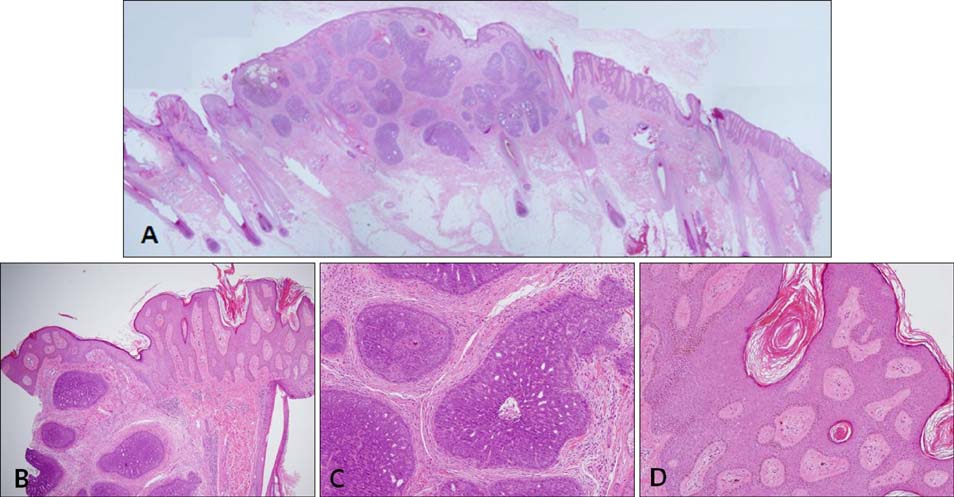
Fig. 2 (A) Scanning view of the excision specimen (H&E, scanning view). (B) Biopsy specimen showing well-circumscribed, various-sized dermal tumor lobules. Prominent hyperkeratosis, acanthosis, papillomatosis, and pseudohorn cysts were seen adjacent to the tumor nodule (H&E, ×20). (C) The lobular aggregation was composed of numerous basaloid epithelial nests and multiple primitive papillary structures with distinct peripheral palisading of nuclei (H&E, ×200). (D) Marked hyperkeratosis, acanthosis, papillomatosis, several horn cysts, and mild basal hyperpigmentation were detected in the epidermis (H&E, ×100).
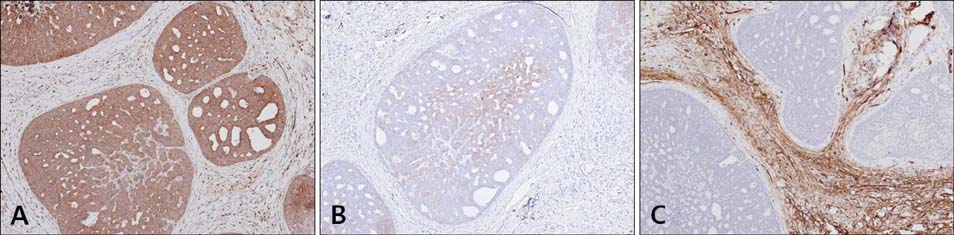
Fig. 3 (A) The entire trichoblastoma tumor lobules were stained against cytokeratin 19 (CK19) monoclonal antibody, showing a mild peripheral palisading of nuclei (×100). (B) Focal tumor cells showed weak CK17 expression (×100). (C) None of the tumor lobules showed immunolabeling against CD34 monoclonal antibody (×100).
Reference
-
1. Headington JT. Differentiating neoplasms of hair germ. J Clin Pathol. 1970; 23:464–471.
Article2. Ackerman AB, DeViragh PA, Chongchitnant N. Neoplasms with follicular differentiation. Philadelphia: Lea and Febiger;1993. p. 401.3. Lee HJ, Choe TJ, Park JG, Ha SJ, Kang SJ, Kim JW. A case of trichoblastoma. Ann Dermatol. 1999; 11:286–288.
Article4. Santos-Briz A, Rodríguez-Peralto JL, Miguélez A, López-Ríos F. Trichoblastoma arising within an apocrine poroma. Am J Dermatopathol. 2002; 24:59–62.
Article5. Battistella M, Peltre B, Cribier B. Composite tumors associating trichoblastoma and benign epidermal/follicular neoplasm: another proof of the follicular nature of inverted follicular keratosis. J Cutan Pathol. 2010; 37:1057–1063.
Article6. Wilson CL, Dean D, Lane EB, Dawber RP, Leigh IM. Keratinocyte differentiation in psoriatic scalp: morphology and expression of epithelial keratins. Br J Dermatol. 1994; 131:191–200.
Article7. Yamamoto O, Asahi M. Cytokeratin expression in trichoblastic fibroma (small nodular type trichoblastoma), trichoepithelioma and basal cell carcinoma. Br J Dermatol. 1999; 140:8–16.
Article8. Johnson WC. Metastatic carcinoma of the skin. In : Elder D, Elenitas R, Jaworsky C, Johnson B, editors. Lever's histopathology of the skin. 10th ed. Philadelphia: Lippincott;2009. p. 1155–1156.9. Kim HJ, Min HG, Lee ES. Alopecia neoplastica in a patient with gastric carcinoma. Br J Dermatol. 1999; 141:1122–1124.
Article10. Kirchmann TT, Prieto VG, Smoller BR. CD34 staining pattern distinguishes basal cell carcinoma from trichoepithelioma. Arch Dermatol. 1994; 130:589–592.
Article11. Conner KB, Cohen PR. Cutaneous metastasis of breast carcinoma presenting as alopecia neoplastica. South Med J. 2009; 102:385–389.
Article12. Kohno A, Saruta T, Kimura H. A case of alopecia neoplastica due to cutaneous metastasis from stomach. Rhinsho Derm. 1983; 25:334–335.13. Yuen YF, Lewis EJ, Larson JT, Wilke MS, Rest EB, Zachary CB. Scalp metastases mimicking alopecia areata. First case report of placental site trophoblastic tumor presenting as cutaneous metastasis. Dermatol Surg. 1998; 24:587–591.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Seborrheic Keratosis with Focal Acantholysis
- A Case of Basal Cell Carcinoma Arising in Seborrheic Keratosis
- Bowen Disease Arising in Recurred Seborrheic Keratosis after Incomplete Removal
- Secondary Localized Cutaneous Amyloidosis in Seborrheic Keratosis
- Eccrine Porocarcinoma associated with Seborrheic Keratosis
