Long-term Complete Response with Lapatinib Plus Capecitabine in a Patient with HER2-Positive Breast Cancer Metastasized to the Pancreas
- Affiliations
-
- 1Department of Internal Medicine, Korea Cancer Center Hospital, Korea Institute of Radiological and Medical Sciences, Seoul, Korea. hyejin@kcch.re.kr
- 2Department of General Surgery, Korea Cancer Center Hospital, Korea Institute of Radiological and Medical Sciences, Seoul, Korea.
- 3Department of Pathology, Korea Cancer Center Hospital, Korea Institute of Radiological and Medical Sciences, Seoul, Korea.
- KMID: 2171353
- DOI: http://doi.org/10.12771/emj.2015.38.3.138
Abstract
- A 37-year-old woman underwent a total mastectomy and adjuvant chemotherapy for HER2-positive breast cancer (pT1N0M), and then recurred in the right lung followed by the pancreas. Lung lobectomy and pylorus-preserving pancreaticoduodenectomy were performed, and systemic chemotherapies including trastuzumab were sequentially administered. However, metastasis to the pancreatic tail was detected. She underwent image-guided radiation therapy, but this was not effective. Lapatinib plus capecitabine combination was administered as forth-line treatment and the metastatic lesion was disappeared. She is continuing this regimen with a complete response for 48 months until now.
Keyword
MeSH Terms
Figure
-
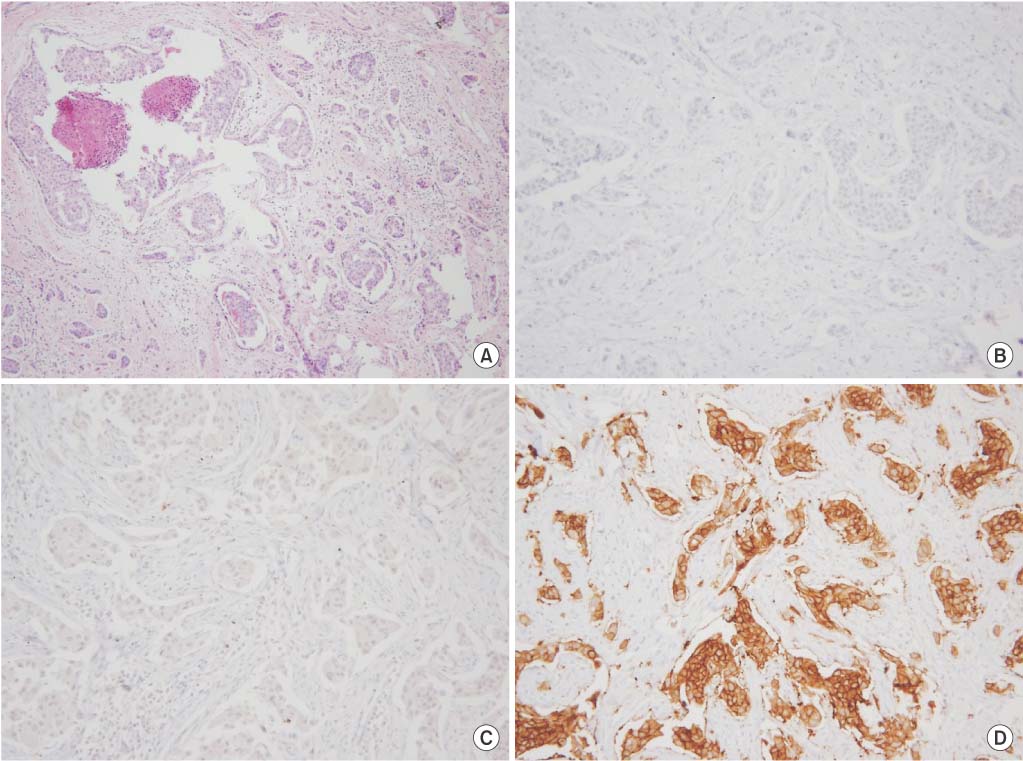
Fig. 1 Microscopic findings of resected specimen. (A) Primary breast cancer is composed of nuclear grade 2 invasive ductal carcinoma and comedo type ductal carcinoma in situ (H&E, ×100). Immunohistochemically, the tumor cells are negative for estrogen receptor (B) and progesterone receptor (C) but positive for C-erbB2 (D) (×200).

Fig. 2 Radiologic and microscopic findings of pulmonary nodule. (A) A chest computed tomography scan shows a single nodule in the lower lobe of the right lung (black arrow). (B) An 18F-fluorodeoxyglucose positron emission tomography computed tomography scan shows no distant metastasis except to the lung. (C) Microscopically, tumor cells are arranged in a nest-like pattern in the alveolar spaces (H&E, ×100). (D) Tumor cells are immunoreactive for C-erbB2 (×200).

Fig. 3 Radiologic and microscopic findings of pancreatic head lesion. (A) An 18F-fluorodeoxyglucose positron emission tomography computed tomography scan shows a hypermetabolic lesion (standardized uptake value, 7.7) in the pancreatic head. (B) This lesion is a low-attenuating mass (1.5 cm) on an abdominal-pelvic computed tomography scan. (C) Microscopically, the tumor cells show a small nest-like pattern with infiltrative features in the fibrous stroma (H&E, ×100). (D) Tumor cells are strongly immunoreactive for C-erbB2 (×200).
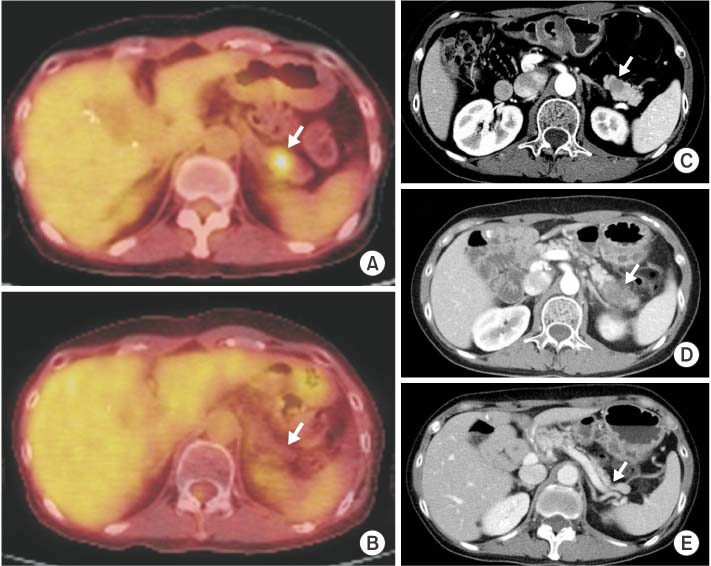
Fig. 4 Radiologic findings of pancreatic tail lesion with complete response. The pancreatic tail mass has been initially shown as a hypermetabolic lesion (standardized uptake value, 3.3) on an 18F-fluorodeoxyglucose positron emission tomography computed tomography (18F-FDG PET-CT) scan (A) and as a low-attenuating lesion (1.5 cm) on an abdominal-pelvic CT scan (C). After image-guided radiation therapy of 45 Gy, enlarged mass is shown (D). However, after combination chemotherapy with lapatinib and capecitabine, this pancreatic tail mass disappeared on 18F-FDG PET-CT (B) and CT (E) scans.
Reference
-
1. Hudis CA. Trastuzumab: mechanism of action and use in clinical practice. N Engl J Med. 2007; 357:39–51.2. Cho HS, Mason K, Ramyar KX, Stanley AM, Gabelli SB, Denney DW Jr, et al. Structure of the extracellular region of HER2 alone and in complex with the Herceptin Fab. Nature. 2003; 421:756–760.3. Tandon AK, Clark GM, Chamness GC, Ullrich A, McGuire WL. HER-2/neu oncogene protein and prognosis in breast cancer. J Clin Oncol. 1989; 7:1120–1128.4. Baselga J, Cortes J, Kim SB, Im SA, Hegg R, Im YH, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med. 2012; 366:109–119.5. Verma S, Miles D, Gianni L, Krop IE, Welslau M, Baselga J, et al. Trastuzumab emtansine for HER2-positive advanced breast cancer. N Engl J Med. 2012; 367:1783–1791.6. Geyer CE, Forster J, Lindquist D, Chan S, Romieu CG, Pienkowski T, et al. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med. 2006; 355:2733–2743.7. Di Lascio S, Pagani O. Oligometastatic breast cancer: a shift from palliative to potentially curative treatment? Breast Care (Basel). 2014; 9:7–14.8. Weichselbaum RR, Hellman S. Oligometastases revisited. Nat Rev Clin Oncol. 2011; 8:378–382.9. Meimarakis G, Ruttinger D, Stemmler J, Crispin A, Weidenhagen R, Angele M, et al. Prolonged overall survival after pulmonary metastasectomy in patients with breast cancer. Ann Thorac Surg. 2013; 95:1170–1180.10. Cifuentes N, Pickren JW. Metastases from carcinoma of mammary gland: an autopsy study. J Surg Oncol. 1979; 11:193–205.11. Bachelot T, Romieu G, Campone M, Dieras V, Cropet C, Dalenc F, et al. Lapatinib plus capecitabine in patients with previously untreated brain metastases from HER2-positive metastatic breast cancer (LANDSCAPE): a single-group phase 2 study. Lancet Oncol. 2013; 14:64–71.12. Suh J, Stea B, Tankel K, Marsiglia H, Belkacemi Y, Gomez H, et al. Results of the phase III ENRICH (RT-016) study of efaproxiral administered concurrent with whole brain radiation therapy (WBRT) in women with brain metastases from breast cancer. Int J Radiat Oncol Biol Phys. 2008; 72:1 Suppl. S50–S51.13. Murphy CG, Morris PG. Recent advances in novel targeted therapies for HER2-positive breast cancer. Anticancer Drugs. 2012; 23:765–776.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Real-World Data of Pyrotinib-Based Therapy in Metastatic HER2-Positive Breast Cancer: Promising Efficacy in Lapatinib-Treated Patients and in Brain Metastasis
- Diagnosis and Treatment of HER2-Positive Breast Cancer
- Effective Treatment of Solitary Pituitary Metastasis with Panhypopituitarism in HER2-Positive Breast Cancer by Lapatinib
- The current status of cancer survivorship care and a consideration of appropriate care model in Korea
- Impact of HER2-Low Status on Pathologic Complete Response and Survival Outcome Among Breast Cancer Patients Undergoing Neoadjuvant Chemotherapy
