Papillary Thyroid Cancer from Lateral Aberrant Thyroid Masquerading as Cervical Metastasis from Larynx Cancer: A Case Report
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Veterans Health Service Medical Center, Seoul, Korea. entzzang1020@daum.net
- 2Department of Pathology, Veterans Health Service Medical Center, Seoul, Korea.
- KMID: 2171228
- DOI: http://doi.org/10.11106/ijt.2015.8.2.190
Abstract
- The aberrant or ectopic thyroid in lateral neck is a rare developmental anomaly. Furthermore, the primary thyroid carcinoma arising in ectopic thyroid is extremely rare, only a few cases have been reported so far in English literature. We report a 64-year-old male with left transglottic cancer and primary papillary carcinoma from lateral aberrant thyroid in left lateral neck. Preoperatively, we diagnosed as transglottic cancer with ipsilateral neck metastasis. The patient underwent total laryngectomy, left selective neck dissection and left thyroidectomy. Finally, the patient was diagnosed as left transglottic cancer and papillary carcinoma from lateral aberrant thyroid. Surgeons should take into account a primary ectopic thyroid carcinoma arising in lateral neck may co-exist with another type of head and neck tumor.
Keyword
MeSH Terms
Figure
-
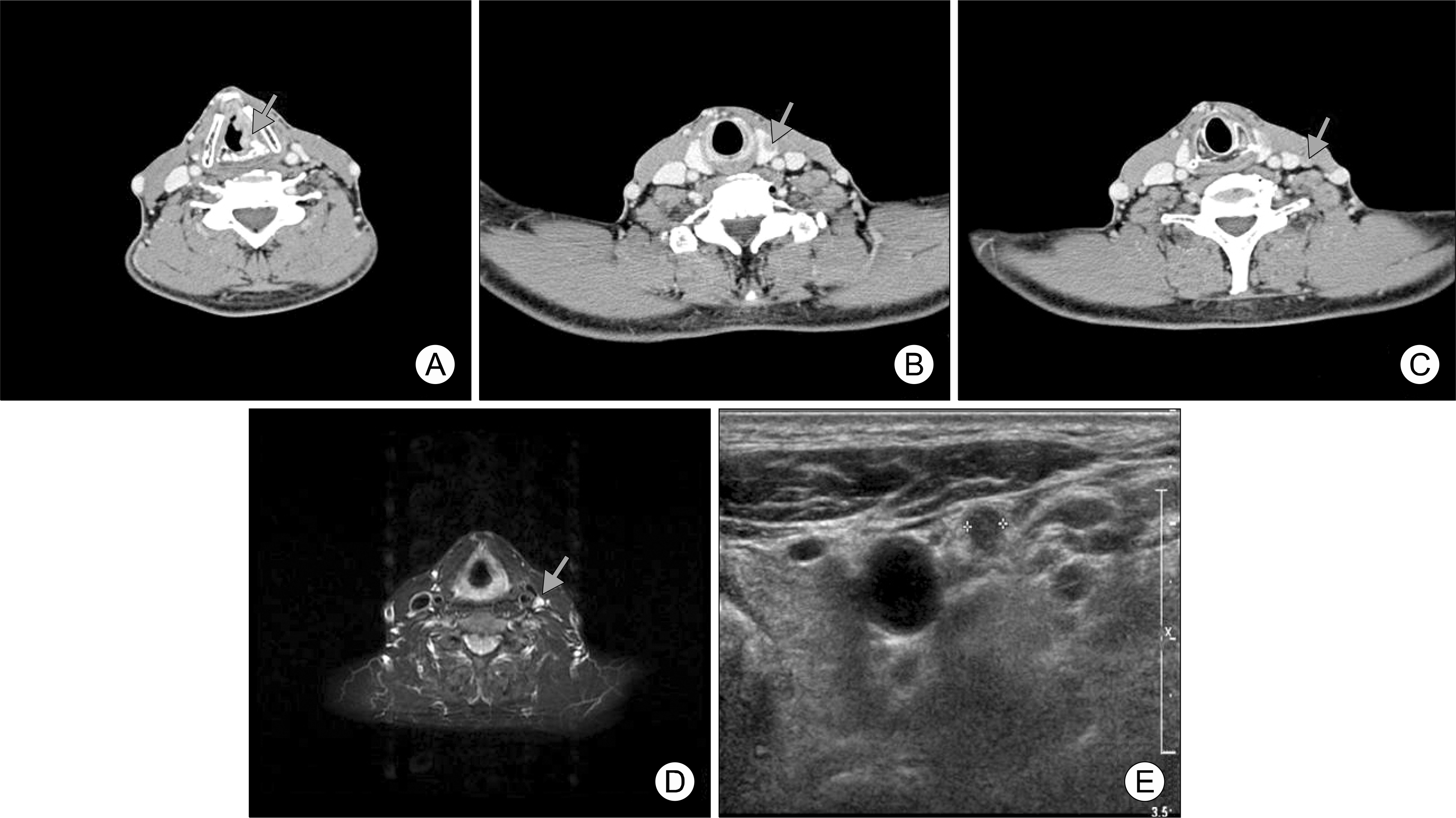
Fig. 1. Preoperative imaging studies. (A) Neck CT scan shows 1.2×2.1 cm sized enhanced soft tissue mass in left true vocal cord (arrow). (B) Neck CT scan shows 1.3×1.2 cm sized nodule in left thyroid gland (arrow). (C) Neck CT scan shows 0.8×0.9 cm sized iso-dense round mass in left level III (arrow). (D) T2-weighted MRI shows slight high signal intensity mass in left level III (arrow). (E) Ultrasonographic image shows about 1×0.8 cm sized ovoid hypoechogenic nodule in the left lateral neck (asterik).
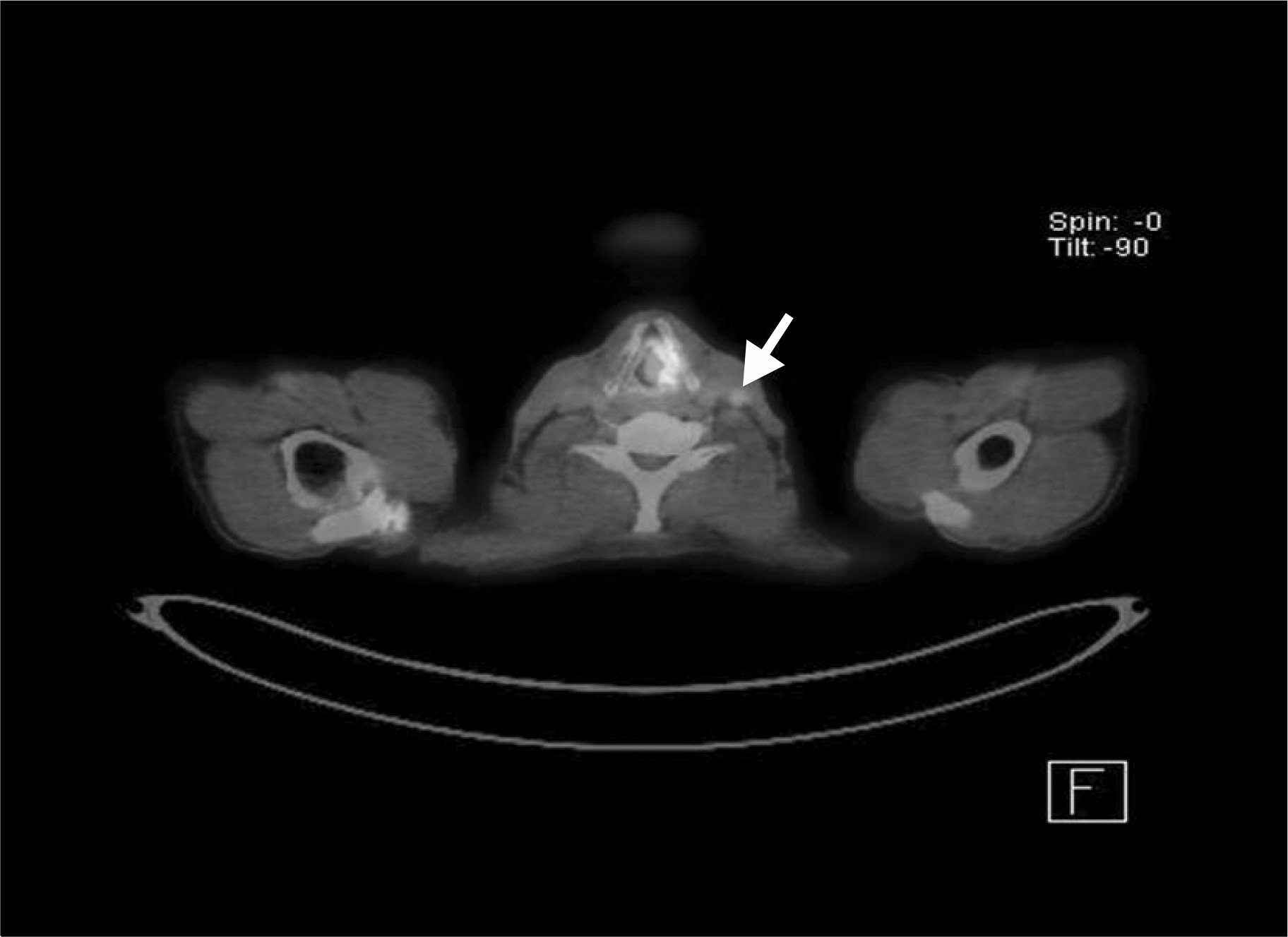
Fig. 2. Preoperative PET CT scans. It shows strong FDG uptake on left vocal cord (standard uptake value, 20.4), mild uptake on left level III (SUV, 2.2) (white arrow).
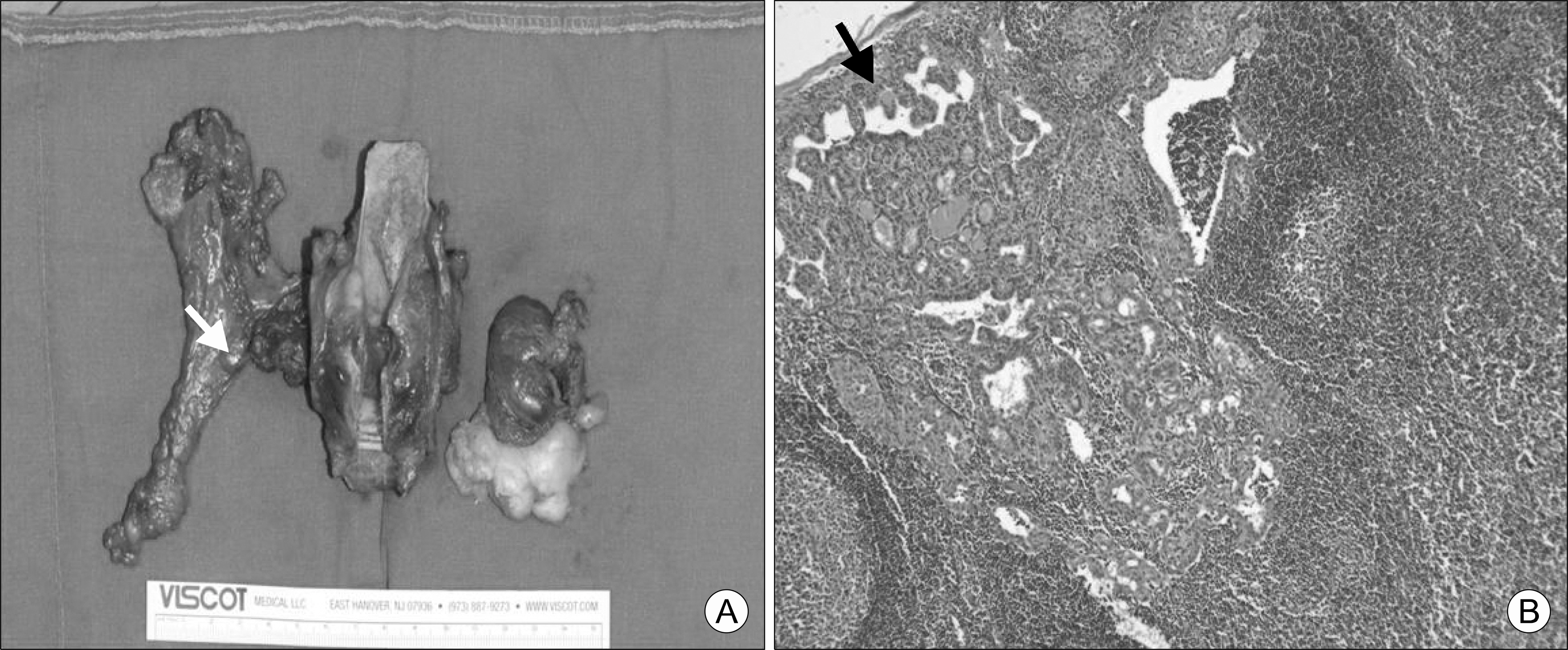
Fig. 3. Pathologic findings. (A) Gross photograph shows the specimen of total laryngectomy with left selective neck dissection and left thyroidectomy. The white arrow indicates small lymph node in level III. (B) Microscopic findings: The fronds of tissue have thin fibrovascular cores and an overall papillary pattern. The black arrow indicates papillary architectures (H&E, ×100).
Reference
-
References
1. Paresi RJ Jr, Shah D. Hashimoto's thyroiditis presenting as an enlarging submandibular mass in a patient with a lingual thyroid. Otolaryngol Head Neck Surg. 2005; 132(5):806–8.
Article2. Huang TS, Chen HY. Dual thyroid ectopia with a normally located pretracheal thyroid gland: case report and literature review. Head Neck. 2007; 29(9):885–8.
Article3. Kang JH, Choi KM, Kim YJ, Kim SW. A case of anaplastic carcinoma arising ectopic thyroid. Korean J Head Neck Oncol. 2009; 25(2):153–5.4. Mansberger AR Jr, Wei JP. Surgical embryology and anatomy of the thyroid and parathyroid glands. Surg Clin North Am. 1993; 73(4):727–46.
Article5. De Felice M, Di Lauro R. Thyroid development and its disorders: genetics and molecular mechanisms. Endocr Rev. 2004; 25(5):722–46.
Article6. Frantz VK, Forsythe R, Hanford JM, Rogers WM. Lateral aberrant thyroids. Ann Surg. 1942; 115(2):161–83.
Article7. Yoon JS, Won KC, Cho IH, Lee JT, Lee HW. Clinical characteristics of ectopic thyroid in Korea. Thyroid. 2007; 17(11):1117–21.
Article8. Barber TW, Lee ST, Lim E, Lim HK, Scott AM. Benign ectopic multinodular thyroid tissue in the submandibular region with a coexistent normotopic multinodular thyroid gland harboring papillary thyroid cancer. Clin Nucl Med. 2010; 35(8):618–9.
Article9. Maceri DR, Babyak J, Ossakow SJ. Lateral neck mass. Sole presenting sign of metastatic thyroid cancer. Arch Otolaryngol Head Neck Surg. 1986; 112(1):47–9.
Article10. Ohnishi H, Sato H, Noda H, Inomata H, Sasaki N. Color Doppler ultrasonography: diagnosis of ectopic thyroid gland in patients with congenital hypothyroidism caused by thyroid dys-genesis. J Clin Endocrinol Metab. 2003; 88(11):5145–9.
Article11. Shah BC, Ravichand CS, Juluri S, Agarwal A, Pramesh CS, Mistry RC. Ectopic thyroid cancer. Ann Thorac Cardiovasc Surg. 2007; 13(2):122–4.12. Cabibi D, Cacciatore M, Guarnotta C, Aragona F. Immunohistochemistry differentiates papillary thyroid carcinoma arising in ectopic thyroid tissue from secondary lymph node metastases. Thyroid. 2007; 17(7):603–7.
Article13. Brindle R, Mullan D, Yap BK, Gandhi A. Thyroid incidentalomas discovered on positron emission tomography CT scanning – Malignancy rate and significance of standardised uptake values. Eur J Surg Oncol. 2014; 40(11):1528–32.
Article14. Shaha AR, Shah JP, Loree TR. Patterns of nodal and distant metastasis based on histologic varieties in differentiated carcinoma of the thyroid. Am J Surg. 1996; 172(6):692–4.
Article15. Seven H, Gurkan A, Cinar U, Vural C, Turgut S. Incidence of occult thyroid carcinoma metastases in lateral cervical cysts. Am J Otolaryngol. 2004; 25(1):11–7.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Papillary Thyroid Cancer Arising in Lateral Aberrant Thyroid Presenting with Multiple Metastases
- A Case of an Ectopic Thyroid Gland at the Lateral Neck Masquerading as a Metastatic Papillary Thyroid Carcinoma
- The Pattern of Cervical Lymph Node Metastases in Papillary Thyroid Cancer
- A Case of Cystic Lymph Node Metastasis from Thyroid Papillary Microcarcinoma
- Thyroid Lobectomy as an Initial Treatment Option on 1-4 cm Papillary Cancer
