Endocrinol Metab.
2016 Mar;31(1):153-160. 10.3803/EnM.2016.31.1.153.
Recovery of Adrenal Function in Patients with Glucocorticoids Induced Secondary Adrenal Insufficiency
- Affiliations
-
- 1Department of Internal Medicine, Gyeongsang National University Hospital, Gyeongsang National University School of Medicine, Jinju, Korea. taesikjung@gmail.com
- 2Institute of Health Sciences, Gyeongsang National University School of Medicine, Jinju, Korea.
- KMID: 2169707
- DOI: http://doi.org/10.3803/EnM.2016.31.1.153
Abstract
- BACKGROUND
The chronic use of glucocorticoids (GC) suppresses function of the hypothalamic-pituitary-adrenal axis and often results in secondary adrenal insufficiency (AI). The present study aimed to determine the recovery rate of adrenal function in patients with secondary AI within 1 to 2 years and to assess the factors predictive of adrenal function recovery.
METHODS
This was a retrospective observational study that enrolled patients diagnosed with GC-induced secondary AI between 2007 and 2013. AI was defined by peak serum cortisol levels <18 µg/dL during a standard-dose short synacthen test (SST). A follow-up SST was performed after 1 to 2 years, and responders were defined as those with adrenocorticotropic hormone (ACTH)-stimulated peak serum cortisol levels ≥18 µg/dL.
RESULTS
Of the total 34 patients diagnosed with GC-induced secondary AI at first, 20 patients (58.8%) recovered normal adrenal function by the time of the follow-up SST (median follow-up period, 16.5 months). Although the baseline serum ACTH and cortisol levels at the first SST did not differ between responders and non-responders, the incremental cortisol response during the first SST was higher in responders than that of non-responders (7.88 vs. 3.56, P<0.01). Additionally, higher cortisol increments during the first SST were an independent predictive factor of the adrenal function recovery (odds ratio, 1.58; 95% confidence interval, 1.02 to 2.46; P<0.05).
CONCLUSION
In the present study, adrenal function recovery was achieved frequently in patients with GC-induced secondary AI within 1 to 2 years. Additionally, an incremental cortisol response at the first SST may be an important predictive factor of adrenal function recovery.
MeSH Terms
Figure
-
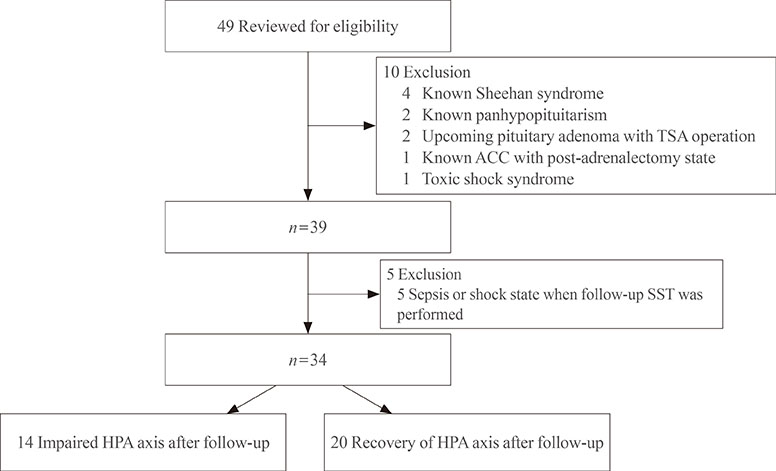
Fig. 1 Subject enrollment. TSA, transshenoidal approach; ACC, adrenal cortical carcinoma; SST, short synacthen test; HPA, hypothalamic-pituitary-adrenal.
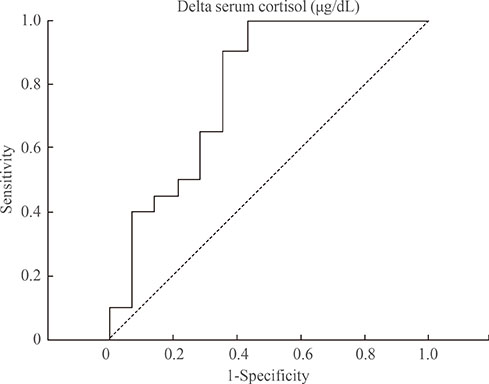
Fig. 2 The area under the receiver operating characteristic curve to assess the ability of the serum cortisol increment (delta cortisol) to predict the hypothalamic-pituitary-adrenal axis recovery after the first short synacthen test. A peak cortisol cut-off of ≥8.15 µg/dL gives a sensitivity of 50% and a specificity of 79%, and that of ≥8.99 µg/dL gives a sensitivity of 40% and a specificity of 86% for predicting adrenal function recovery.
Reference
-
1. Fardet L, Petersen I, Nazareth I. Description of oral glucocorticoid prescriptions in general population. Rev Med Interne. 2011; 32:594–599.2. Walsh LJ, Wong CA, Pringle M, Tattersfield AE. Use of oral corticosteroids in the community and the prevention of secondary osteoporosis: a cross sectional study. BMJ. 1996; 313:344–346.3. Gudbjornsson B, Juliusson UI, Gudjonsson FV. Prevalence of long term steroid treatment and the frequency of decision making to prevent steroid induced osteoporosis in daily clinical practice. Ann Rheum Dis. 2002; 61:32–36.4. Overman RA, Yeh JY, Deal CL. Prevalence of oral glucocorticoid usage in the United States: a general population perspective. Arthritis Care Res (Hoboken). 2013; 65:294–298.5. Kim KM, Kim BR, Lee JS, Han OY, Park MS, Yim HW, et al. A survey on pharmacists' prescription behaviors for topical steroids in regions without separation of dispensary from medical practice in Korea. Korean J Clin Pharm. 2011; 21:161–169.6. Lee C, Shin E, Park S, Kim H, Kim W. Performance evaluation for ten-years of government separation policy on prescription and dispensing of drugs: a literature review study. Health Policy Manage. 2013; 23:188–195.7. Liu D, Ahmet A, Ward L, Krishnamoorthy P, Mandelcorn ED, Leigh R, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013; 9:30.8. Jasani MK, Boyle JA, Greig WR, Dalakos TG, Browning MC, Thompson A, et al. Corticosteroid-induced suppression of the hypothalamo-pituitary-adrenal axis: observations on patients given oral corticosteroids for rheumatoid arthritis. Q J Med. 1967; 36:261–276.9. Venkatesh B, Cohen J. The utility of the corticotropin test to diagnose adrenal insufficiency in critical illness: an update. Clin Endocrinol (Oxf). 2015; 83:289–297.10. Bornstein SR. Predisposing factors for adrenal insufficiency. N Engl J Med. 2009; 360:2328–2339.11. Gleeson HK, Walker BR, Seckl JR, Padfield PL. Ten years on: safety of short synacthen tests in assessing adrenocorticotropin deficiency in clinical practice. J Clin Endocrinol Metab. 2003; 88:2106–2111.12. Arlt W. The approach to the adult with newly diagnosed adrenal insufficiency. J Clin Endocrinol Metab. 2009; 94:1059–1067.13. Agha A, Tomlinson JW, Clark PM, Holder G, Stewart PM. The long-term predictive accuracy of the short synacthen (corticotropin) stimulation test for assessment of the hypothalamic-pituitary-adrenal axis. J Clin Endocrinol Metab. 2006; 91:43–47.14. Livanou T, Ferriman D, James VH. Recovery of hypothalamo-pituitary-adrenal function after corticosteroid therapy. Lancet. 1967; 2:856–859.15. Tempark T, Phatarakijnirund V, Chatproedprai S, Watcharasindhu S, Supornsilchai V, Wananukul S. Exogenous Cushing's syndrome due to topical corticosteroid application: case report and review literature. Endocrine. 2010; 38:328–334.16. Graber AL, Ney RL, Nicholson WE, Island DP, Liddle GW. Natural history of pituitary-adrenal recovery following long-term suppression with corticosteroids. J Clin Endocrinol Metab. 1965; 25:11–16.17. Henzen C, Suter A, Lerch E, Urbinelli R, Schorno XH, Briner VA. Suppression and recovery of adrenal response after short-term, high-dose glucocorticoid treatment. Lancet. 2000; 355:542–545.18. Broersen LH, Pereira AM, Jorgensen JO, Dekkers OM. Adrenal insufficiency in corticosteroids use: systematic review and meta-analysis. J Clin Endocrinol Metab. 2015; 100:2171–2180.19. LaRochelle GE Jr, LaRochelle AG, Ratner RE, Borenstein DG. Recovery of the hypothalamic-pituitary-adrenal (HPA) axis in patients with rheumatic diseases receiving low-dose prednisone. Am J Med. 1993; 95:258–264.20. Berr CM, Di Dalmazi G, Osswald A, Ritzel K, Bidlingmaier M, Geyer LL, et al. Time to recovery of adrenal function after curative surgery for Cushing's syndrome depends on etiology. J Clin Endocrinol Metab. 2015; 100:1300–1308.21. Yo WS, Toh LM, Brown SJ, Howe WD, Henley DE, Lim EM. How good is a morning cortisol in predicting an adequate response to intramuscular synacthen stimulation? Clin Endocrinol (Oxf). 2014; 81:19–24.22. Jamilloux Y, Liozon E, Pugnet G, Nadalon S, Heang Ly K, Dumonteil S, et al. Recovery of adrenal function after long-term glucocorticoid therapy for giant cell arteritis: a cohort study. PLoS One. 2013; 8:e68713.23. Wood JB, Frankland AW, James VH, Landon J. A rapid test of adrenocortical function. Lancet. 1965; 1:243–245.24. Stewart PM, Corrie J, Seckl JR, Edwards CR, Padfield PL. A rational approach for assessing the hypothalamo-pituitary-adrenal axis. Lancet. 1988; 1:1208–1210.25. Plumpton FS, Besser GM, Cole PV. Corticosteroid treatment and surgery. 1. An investigation of the indications for steroid cover. Anaesthesia. 1969; 24:3–11.26. Baruah MP. Sub-clinical addison's disease. Indian J Endocrinol Metab. 2012; 16:Suppl 2. S176–S177.27. Widmer IE, Puder JJ, Konig C, Pargger H, Zerkowski HR, Girard J, et al. Cortisol response in relation to the severity of stress and illness. J Clin Endocrinol Metab. 2005; 90:4579–4586.28. Marik PE, Pastores SM, Annane D, Meduri GU, Sprung CL, Arlt W, et al. Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: consensus statements from an international task force by the American College of Critical Care Medicine. Crit Care Med. 2008; 36:1937–1949.29. Klose M, Lange M, Rasmussen AK, Skakkebaek NE, Hilsted L, Haug E, et al. Factors influencing the adrenocorticotropin test: role of contemporary cortisol assays, body composition, and oral contraceptive agents. J Clin Endocrinol Metab. 2007; 92:1326–1333.30. Schlaghecke R, Kornely E, Santen RT, Ridderskamp P. The effect of long-term glucocorticoid therapy on pituitary-adrenal responses to exogenous corticotropin-releasing hormone. N Engl J Med. 1992; 326:226–230.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis and Treatment of Adrenal Insufficiency
- Adrenocortical Insufficiency due to Spontaneous Bilateral Adrenal Hemorrhage Presented as Acute Abdominal Pain
- A Case of Rifampin-Induced Recurrent Adrenal Insufficiency During the Treatment of Pulmonary Tuberculosis in a Patient with Addison's Disease
- A Case of Addison's Disease: Partial Recovery of Adrenocortical Function Following Antituberculous Medication
- Adrenal Tuberculosis Mimicking a Malignant Tumor with Primary Adrenal Insufficiency
