Endocrinol Metab.
2011 Dec;26(4):317-323. 10.3803/EnM.2011.26.4.317.
Clinical Characteristics of Patients with Hyperglycemic Emergency State Accompanying Rhabdomyolysis
- Affiliations
-
- 1Department of Internal Medicine, Gyeongsang National University School of Medicine, Jinju, Korea. taesikjung@gmail.com
- 2Institute of Health Sciences, Gyeongsang National University School of Medicine, Jinju, Korea.
- KMID: 2169262
- DOI: http://doi.org/10.3803/EnM.2011.26.4.317
Abstract
- BACKGROUND
The purpose of this study was to investigate the prevalence of rhabdomyolysis and its association with both clinical course and prognosis and to evaluate the factors associated with rhabdomyolysis in patients with hyperglycemic emergencies.
METHODS
We reviewed the medical records of patients with hyperglycemic emergencies who visited our hospital from May 2003 to April 2010. We assessed the clinical characteristics, biochemical profiles and clinical course of patients and analyzed these data according to the presence of rhabdomyolysis.
RESULTS
The prevalence of rhabdomyolysis was 29 patients (28.4%) among 102 patients. Mean serum osmolarity, glucose and serum creatinine levels were higher in patients with rhabdomyolysis than those without rhabdomyolysis. Patients with rhabdomyolysis had higher rates of hemodialysis and mortality than those without the condition. The factors associated with rhabdomyolysis in the hyperglycemic emergency state were increased serum osmolarity and APACHE II score on admission (P < 0.05).
CONCLUSION
Rhabdomyolysis commonly occurred in patients with hyperglycemic emergencies and this could aggravate their clinical course and increase mortality.
MeSH Terms
Figure
-
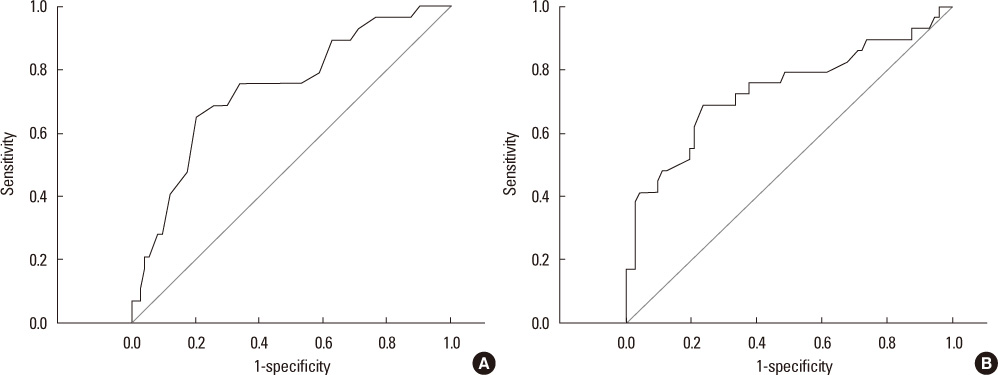
Fig. 1 Receiver operating characteristic curves for the prediction of the occurrence of rhabdomyolysis in hyperglycemic emergency state. A. Acute physiology and chronic health evaluation (APACHE) II score. B. Serum osmolality.
Reference
-
1. Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN. Hyperglycemic crises in adult patients with diabetes. Diabetes Care. 2009. 32:1335–1343.2. Trachtenbarg DE. Diabetic ketoacidosis. Am Fam Physician. 2005. 71:1705–1714.3. Kitabchi AE, Nyenwe EA. Hyperglycemic crises in diabetes mellitus: diabetic ketoacidosis and hyperglycemic hyperosmolar state. Endocrinol Metab Clin North Am. 2006. 35:725–751.4. Stoner GD. Hyperosmolar hyperglycemic state. Am Fam Physician. 2005. 71:1723–1730.5. Nugent BW. Hyperosmolar hyperglycemic state. Emerg Med Clin North Am. 2005. 23:629–648.6. MacIsaac RJ, Lee LY, McNeil KJ, Tsalamandris C, Jerums G. Influence of age on the presentation and outcome of acidotic and hyperosmolar diabetic emergencies. Intern Med J. 2002. 32:379–385.7. Wachtel TJ, Tetu-Mouradjian LM, Goldman DL, Ellis SE, O'Sullivan PS. Hyperosmolarity and acidosis in diabetes mellitus: a three-year experience in Rhode Island. J Gen Intern Med. 1991. 6:495–502.8. Huerta-Alardín AL, Varon J, Marik PE. Bench-to-bedside review: rhabdomyolysis -- an overview for clinicians. Crit Care. 2005. 9:158–169.9. Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009. 361:62–72.10. Singhal PC, Abramovici M, Ayer S, Desroches L. Determinants of rhabdomyolysis in the diabetic state. Am J Nephrol. 1991. 11:447–450.11. Wang LM, Tsai ST, Ho LT, Hu SC, Lee CH. Rhabdomyolysis in diabetic emergencies. Diabetes Res Clin Pract. 1994. 26:209–214.12. Izumi T, Shimizu E, Imakiire T, Kikuchi Y, Oshima S, Kubota T, Hakozaki Y. A successfully treated case of hyperosmolar hyperglycemic state complicated with rhabdomyolysis, acute kidney injury, and ischemic colitis. Intern Med. 2010. 49:2321–2326.13. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985. 13:818–829.14. Vanholder R, Sever MS, Erek E, Lameire N. Rhabdomyolysis. J Am Soc Nephrol. 2000. 11:1553–1561.15. Lord GM, Scott J, Pusey CD, Rees AJ, Walport MJ, Davies KA, Bulpitt C, Bloom SR, Muntoni FM. Diabetes and rhabdomyolysis. A rare complication of a common disease. BMJ. 1993. 307:1126–1128.16. Møller-Petersen J, Andersen PT, Hjørne N, Ditzel J. Nontraumatic rhabdomyolysis during diabetic ketoacidosis. Diabetologia. 1986. 29:229–234.17. Leung CB, Li PK, Lui SF, Lai KN. Acute renal failure (ARF) caused by rhabdomyolysis due to diabetic hyperosmolar nonketotic coma: a case report and literature review. Ren Fail. 1992. 14:81–85.18. Oken DE, Arce ML, Wilson DR. Glycerol-induced hemoglobinuric acute renal failure in the rat. I. Micropuncture study of the development of oliguria. J Clin Invest. 1966. 45:724–735.19. Chen HF, Wang CY, Lee HY, See TT, Chen MH, Jiang JY, Lee MT, Li CY. Short-term case fatality rate and associated factors among inpatients with diabetic ketoacidosis and hyperglycemic hyperosmolar state: a hospital-based analysis over a 15-year period. Intern Med. 2010. 49:729–737.20. Lee JI, Sohn TS, Chang SA, Lee JM, Cha BY, Son HY, Son HS. Clinical characteristics and outcomes of diabetic ketoacidosis at a single institution. Korean Diabetes J. 2008. 32:165–170.21. Ko SH, Lee WY, Lee JH, Kwon HS, Lee JM, Kim SR, Moon SD, Song KH, Han JH, Ahn YB, Yoo SJ, Son HY. Clinical characteristics of diabetic ketoacidosis in Korea over the past two decades. Diabet Med. 2005. 22:466–469.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Acute Renal Failure Caused by Hyperosmolar Hyperglycemic State Induced-Rhabdomyolysis
- Clinical and Biochemical Characteristics of Elderly Patients With Hyperglycemic Emergency State at a Single Institution
- Newly Diagnosed Diabetes Mellitus With Pancreatic Cancer Manifested as Hyperglycemic Hyperosmolar State
- Rhabdomyolysis due to Sunburn
- Diabetic Ketoacidosis with Hyperglycemic Hyperosmolar State at the Onset of Type 2 Diabetes Mellitus in an Adolescent Male
