Intrathyroidal Metastasis of Lung Adenocarcinoma Presenting as Subacute Thyroiditis
- Affiliations
-
- 1Department of Endocrinology and Metabolism, College of Medicine, Dankook University, Cheonan, Korea. chkendo@dankook.ac.kr
- 2Department of Pathology, College of Medicine, Dankook University, Cheonan, Korea.
- KMID: 2169065
- DOI: http://doi.org/10.3803/EnM.2010.25.3.226
Abstract
- One of the rare diseases for differential diagnosis of subacute thyroiditis is metastases within the thyroid gland. We report here on a 72-year-old-woman with painful goiter and signs of hyperthyroidism. Her serum concentration of thyroid hormone was in the upper limit of normal, and the uptake of radioactive iodine by the thyroid was completely depressed. Although subacute thyroiditis was suspected, an additional work up that included a chest CT scan was done for the combined cough and chronic weakness. The result was lung cancer with metastatic involvement of the thyroid and multiple lymph nodes. She refused further anti-cancer therapy and died 5 months after the diagnosis. For the differential diagnosis of such a rare case, careful examination is important even in patients with the typical symptoms and laboratory findings of subacute thyroiditis.
Keyword
MeSH Terms
Figure
-
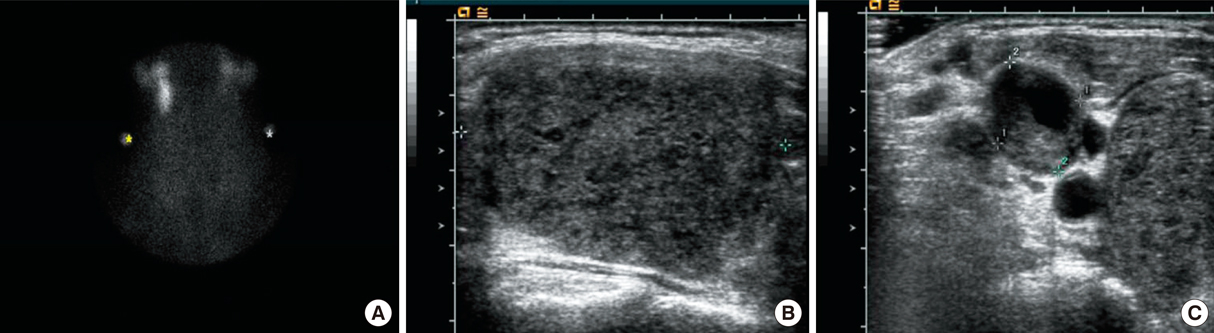
Fig. 1 Thyroid scan and ultrasonography findings. A. 99mTc thyroid scan showed markedly decreased uptake in thyroid area. There was a focal hot uptake lesion below right submandibular gland, too. B. Ultrasonography showed marked and diffuse enlargement with heterogeneous echo texture of both thyroid glands. Mass like lesions (Rt. 3.66 × 2.90 × 4.72 cm, Lt. 1.89 × 2.36 × 4.34 cm) occupied almost all thyroid parenchyma. C. Multiple lymph nodes enlargements (largest one 1.32 × 1.56 cm) were found in neck ultrasonography along the internal jugular chain, containing internal necrotic portion.

Fig. 2 Simple chest X-ray and CT scan findings. A. Simple radiography of the chest showed well defined mass lesion in right upper lung field and calcified nodular lesion in left lung, apex field. B. Chest CT scan showed 4.2 × 3.7 cm sized mass in right upper lobe posterior segment, and emphysema in both lungs field. C. Heterogeneous enlargement of thyroid and enlarged lymph nodes in right level III, left level III and right IV, right supraclavicular, right upper and lower paratracheal, right interlobar and left lower lobar nodal stations were found.
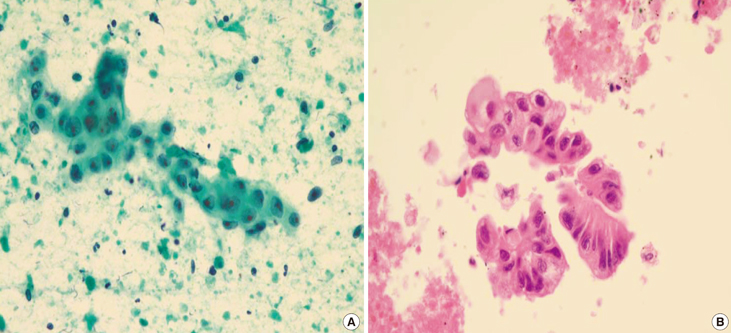
Fig. 3 Thyroid and lung aspiration cytology findings. A. Fine needle aspiration smear of thyroid revealed a cohesive cluster of malignant cells in the markedly necrotic background. The nuclei were oval to round with fine chromatic and single or multiple prominent nucleoli. × 400 Papanicolaou stain. B. Fine needle aspiration (cell block) of lung reveals a cluster of malignant cells very similar to the cells seen in A. The cytoplasm is columnar with mucinous vacuoles and clusters of malignant cells forming rosettes or palisading arrangement. × 400 Hematoxylin-eosin stain.
Reference
-
2. Rosen IB, Strawbridge HG, Walfish PG, Bain J. Malignant pseudothyroiditis: a new clinical entity. Am J Surg. 1978. 136:445–449.3. Liang HH, Wu CH, Tam KW, Chai CY, Lin SE, Chen SC. Thyroid metastasis in a patient with hepatocellular carcinoma: case report and review of literature. World J Surg Oncol. 2007. 5:144.4. Karapanagiotou E, Saif MW, Rondoyianni D, Markaki S, Alamara C, Kiagia M, Pantazopoulus K, Tzannou I, Syrigos K. Metastatic cervical carcinoma to the thyroid gland: a case repost and review of the literature. Yale J Biol Med. 2006. 79:165–168.5. Kim SG, Yang SJ, Kim HY, Seo JA, Baik SH, Bae JW, Choi DS. Malignant pseudothyroiditis induced by thyroid metastasis of rectal cancer. Thyroid. 2007. 17:589–590.6. Watts NB, Sewell CW. Carcinomatous involvement of the thyroid presenting as subacute thyroiditis. Am J Med Sci. 1988. 296:126–128.7. Trokoudes KM, Rosen IB, Strawbridge HT, Bain J. Carconimatous pseudothyroiditis: a problem in differential diagnosis. Can Med Assoc J. 1978. 119:896–898.8. Hamburger JI. The various presentations of thyroiditis: Diagnostic considerations. Ann Intern Med. 1986. 104:219–224.9. Papi G, Fadda G, Corsello SM, Corrado S, Ross ED, Radighieri E, Miraglia A, Carani C, Pontecorvi A. Metastases to the thyroid gland: prevalence, clinicopathological aspects and prognosis: a 10-year experience. Clin Endocrinol (Oxf). 2007. 66:565–571.10. Kim TY, Kim WB, Gong G, Hong SJ, Shong YK. Metastasis to the thyroid diagnosis by fine-needle aspiration biopsy. Clin Endocrinol (Oxf). 2005. 62:236–241.11. Lin JD, Weng HF, Ho YS. Clinical and pathological characteristics of secondary thyroid cancer. Thyroid. 1998. 8:149–153.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cutaneous Metastasis Presenting as an Indurated Plaque Preceding the Diagnosis of Lung Adenocarcinoma
- A Case of Graves' Disease Following Subacute Thyroiditis
- A Case of Riedel's Thyroiditis in a Patient with a History of Subacute Thyroiditis
- Intrathyroidal metastasis of tonsillar squamous cell carcinoma masquerading as a primary thyroid tumor
- A Case of Subacute Thyroiditis Associated with Papillary Thyroid Carcinoma and Takayasu's Arteritis
