Bilateral and pseudobilateral tonsilloliths: Three dimensional imaging with cone-beam computed tomography
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Kirikkale University, Kirikkale, Turkey. m_zahit@hotmail.com
- 2Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Ankara University, Ankara, Turkey.
- KMID: 2167453
- DOI: http://doi.org/10.5624/isd.2013.43.3.163
Abstract
- PURPOSE
Tonsilloliths are calcifications found in the crypts of the palatal tonsils and can be detected on routine panoramic examinations. This study was performed to highlight the benefits of cone-beam computed tomography (CBCT) in the diagnosis of tonsilloliths appearing bilaterally on panoramic radiographs.
MATERIALS AND METHODS
The sample group consisted of 7 patients who had bilateral radiopaque lesions at the area of the ascending ramus on panoramic radiographs. CBCT images for every patient were obtained from both sides of the jaw to determine the exact locations of the lesions and to rule out other calcifications. The calcifications were evaluated on the CBCT images using Ez3D2009 software. Additionally, the obtained images in DICOM format were transferred to ITK SNAP 2.4.0 pc software for semiautomatic segmentation. Segmentation was performed using contrast differences between the soft tissues and calcifications on grayscale images, and the volume in mm3 of the segmented three dimensional models were obtained.
RESULTS
CBCT scans revealed that what appeared on panoramic radiographs as bilateral images were in fact unilateral lesions in 2 cases. The total volume of the calcifications ranged from 7.92 to 302.5mm3. The patients with bilaterally multiple and large calcifications were found to be symptomatic.
CONCLUSION
The cases provided the evidence that tonsilloliths should be considered in the differential diagnosis of radiopaque masses involving the mandibular ramus, and they highlight the need for a CBCT scan to differentiate pseudo- or ghost images from true bilateral pathologies.
MeSH Terms
Figure
-

Fig. 1 A. Selection of reference points in the area of interest is performed. B. ITK-SNAP software allows semiautomatic segmentation of calcifications.

Fig. 2 The CBCT images show a patient with multiple calcifications. Every calcification can be segmented with a different color with ITK-SNAP software.
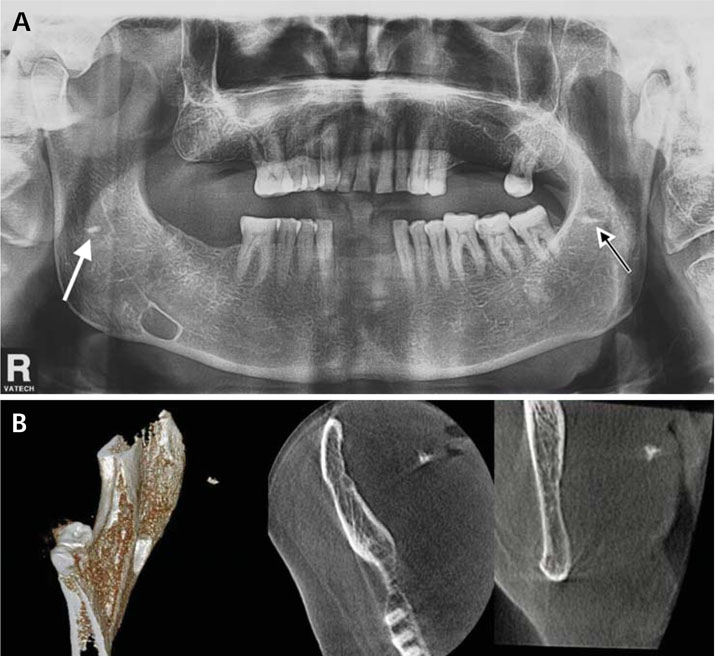
Fig. 3 A. The panoramic radiograph shows a patient with a pseudo-bilateral tonsillolith. The white arrow shows a unilateral calcification that overlapped the middle portion of the ascending ramus. The white and black arrow indicates a ghost image of the radiopacity on the right side appearing higher and more blurred than its source on the left side. B. The CBCT images reveal what appeared on panoramic radiographs as bilateral images were in fact unilateral lesions. The 3D, axial, and coronal CBCT images show a unilateral mass of the right side.
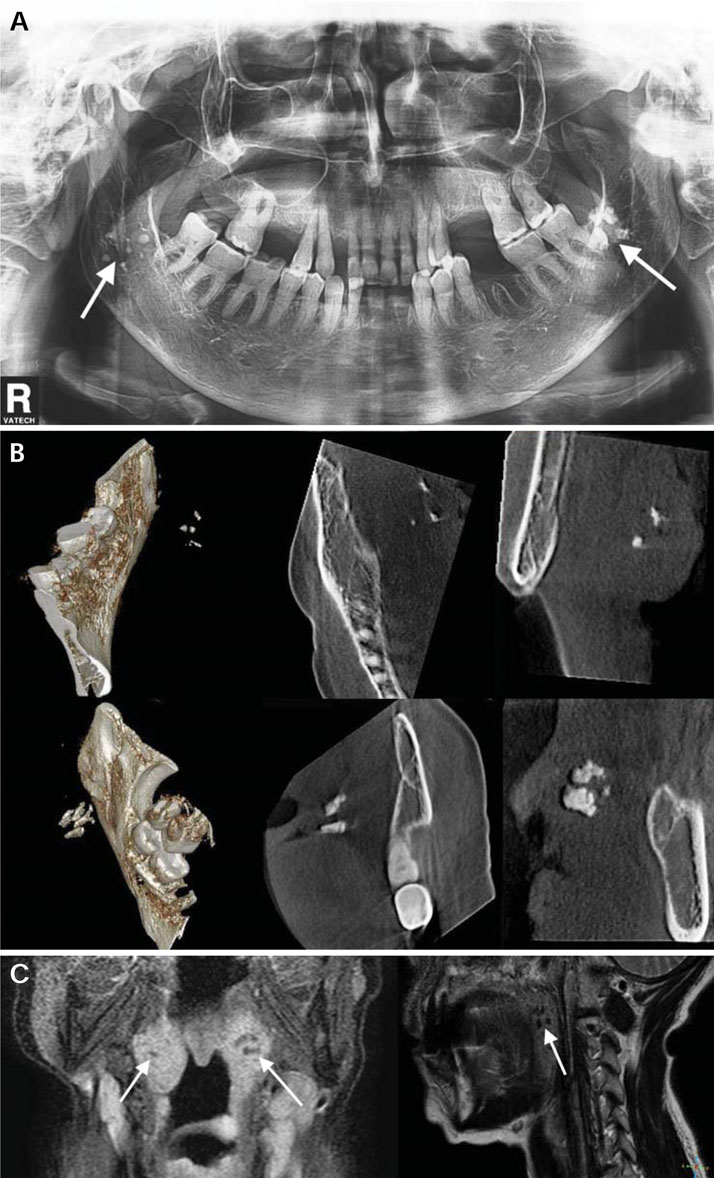
Fig. 4 Case 1. Panoramic, CBCT, and MR images. A. The panoramic radiograph show bilateral calcifications overlapping the middle portion of the ascending ramus, which suggest benign, intra-osseous lesions (white arrows). B. The 3D, axial, and coronal (both sides) CBCT images show bilateral masses in the area of the tonsils. C. The MR images of the same patient show the calcifications in the tonsils (white arrows).

Fig. 5 A. The panoramic radiograph of a patient shows bilateral tonsilloliths. The white and black arrow indicates that some of the radiopaque images on the right side, which do not overlap the ramus, led to a probable diagnosis of soft-tissue calcification. B. CBCT images revealed that they were ghost images of radiopacities on the left side.
Reference
-
1. Silvestre-Donat FJ, Pla-Mocholi A, Estelles-Ferriol E, Martinez-Mihi V. Giant tonsillolith: report of a case. Med Oral Patol Oral Cir Bucal. 2005; 10:239–242.2. Neville B, Damm DD, Allen CM, Bouquot J. Oral & maxillofacial pathology. 2nd ed. Philadelphia: WB Saunders;2002.3. Mesolella M, Cimmino M, Di Martino M, Criscuoli G, Albanese L, Galli V. Tonsillolith. Case report and review of the literature. Acta Otorhinolaryngol Ital. 2004; 24:302–307.4. Ram S, Siar CH, Ismail SM, Prepageran N. Pseudo bilateral tonsilloliths: a case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98:110–114.
Article5. Ozcan E, Ural A, Oktemer TK, Alpaslan G. Bilateral tonsillolithiasis: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:e17–e18.6. Sezer B, Tugsel Z, Bilgen C. An unusual tonsillolith. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 95:471–473.
Article7. Lo RH, Chang KP, Chu ST. Upper airway obstruction caused by bilateral giant tonsilloliths. J Chin Med Assoc. 2011; 74:329–331.
Article8. Poeschl PW, Schmidt N, Guevara-Rojas G, Seemann R, Ewers R, Zipko HT, et al. Comparison of cone-beam and conventional multislice computed tomography for image-guided dental implant planning. Clin Oral Investig. 2013; 17:317–324.
Article9. Pauwels R, Beinsberger J, Stamatakis H, Tsiklakis K, Walker A, Bosmans H, et al. Comparison of spatial and contrast resolution for cone-beam computed tomography scanners. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012; 114:127–135.
Article10. Guevara C, Mandel L. Panoramic radiographic demonstration of bilateral tonsilloliths. N Y State Dent J. 2011; 77:28–30.11. White SC, Pharoah MJ. Oral Radiology: principles and interpretation. 5th ed. St. Louis: Mosby;2004.12. Yasuda CL, Costa AL, Franca M Jr, Pereira FR, Tedeschi H, de Oliveira E, et al. Postcraniotomy temporalis muscle atrophy: a clinical, magnetic resonance imaging volumetry and electromyographic investigation. J Orofac Pain. 2010; 24:391–397.13. Cevidanes LH, Styner MA, Proffit WR. Image analysis and superimposition of 3-dimensional cone-beam computed tomography models. Am J Orthod Dentofacial Orthop. 2006; 129:611–618.
Article14. Cevidanes LH, Bailey LJ, Tucker GR Jr, Styner MA, Mol A, Phillips CL, et al. Superimposition of 3D cone-beam CT models of orthognathic surgery patients. Dentomaxillofac Radiol. 2005; 34:369–375.
Article15. Cooper MM, Steinberg JJ, Lastra M, Antopol S. Tonsillar calculi. Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol. 1983; 55:239–243.16. Marshall WG, Irwin ND. Tonsilloliths. Oral Surg Oral Med Oral Pathol. 1981; 51:113.
Article17. de Moura MD, Madureira DF, Noman-Ferreira LC, Abdo EN, de Aguiar EG, Freire AR. Tonsillolith: a report of three clinical cases. Med Oral Patol Oral Cir Bucal. 2007; 12:E130–E133.18. Almog DM, Horev T, Illig KA, Green RM, Carter LC. Correlating carotid artery stenosis detected by panoramic radiography with clinically relevant carotid artery stenosis determined by duplex ultrasound. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002; 94:768–773.
Article19. Fanibunda K, Lovelock DJ. Calcified stylohyoid ligament: unusual pressure symptoms. Dentomaxillofac Radiol. 1997; 26:249–251.
Article20. Ravon NA, Hollender LG, McDonald V, Persson GR. Signs of carotid calcification from dental panoramic radiographs are in agreement with Doppler sonography results. J Clin Periodontol. 2003; 30:1084–1090.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Three-dimensional imaging modalities in endodontics
- A rare case of dilated invaginated odontome with talon cusp in a permanent maxillary central incisor diagnosed by cone beam computed tomography
- Basic principle of cone beam computed tomography
- Isolated tympanic plate fracture detected by cone-beam computed tomography: report of four cases with review of literature
- CBCT findings of periapical cemento-osseous dysplasia: A case report
