A Case of Huge Lingual Tonsillar Hypertrophy Causing Obstructive Sleep Apnea in Adult
- Affiliations
-
- 1Department of Otorhinolaryngology-Head & Neck Surgery, Dankook University College of Medicine, Cheonan, Korea. lsj72@dankook.ac.kr
- KMID: 2165157
- DOI: http://doi.org/10.18787/jr.2016.23.1.60
Abstract
- Obstructive sleep apnea is characterized by repeated episodes of obstructive apnea and hypopnea. Lingual tonsillar hypertrophy causing obstructive symptoms is a rare disease in adults. Recently, we experienced a case of obstructive sleep apnea due to massive lingual tonsillar hypertrophy. The patient had tonsillectomy as a child and underwent adenoidectomy three years prior to the current presentation due to snoring and sleep apnea. However, symptoms did not improve and were recently aggravated. The upper airway evaluation and polysomnography revealed excessive lingual tonsillar hypertrophy and severe obstructive sleep apnea. An enlarged lingual tonsil was successfully removed using a Coblator. No recurrence was observed, and the obstructive sleep apnea was resolved postoperatively.
Keyword
MeSH Terms
Figure
-
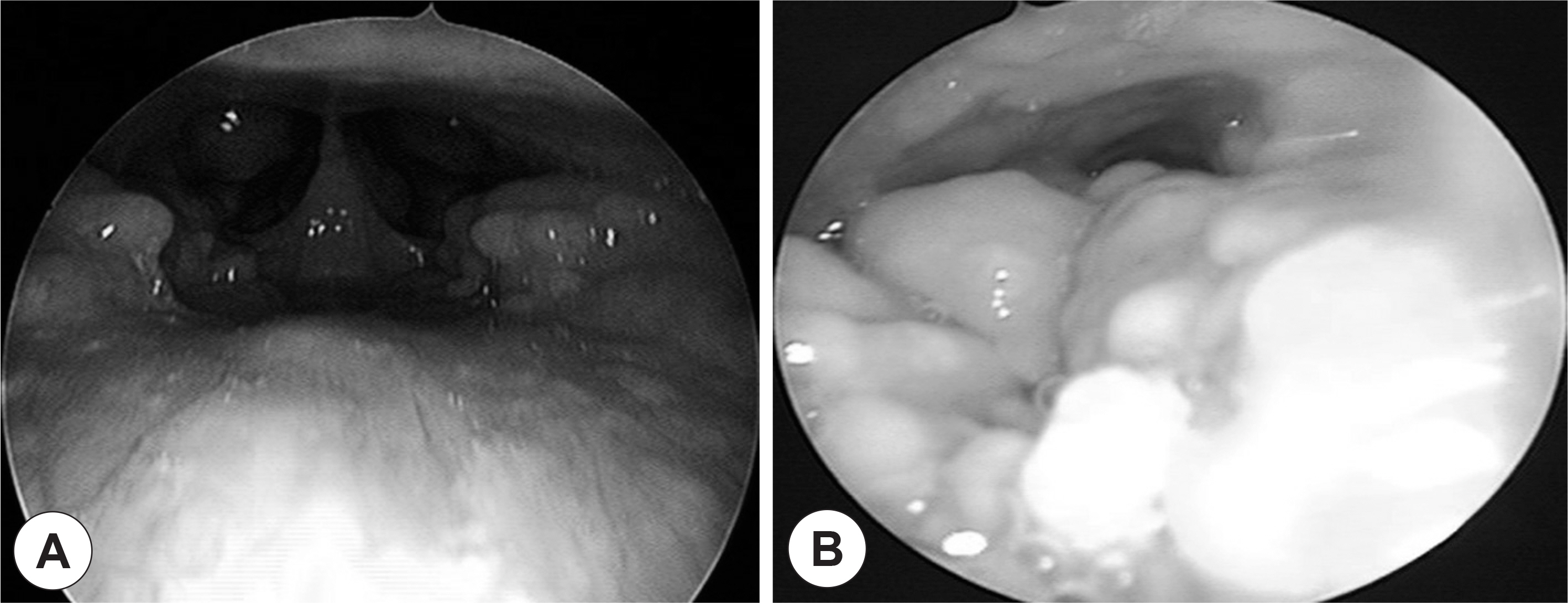
Fig. 1. Preoperative endoscopic findings. Nasopharyngeal airway was patent with mild tubal tonsillar hypertrophy around eustachian tube orifice (A). Enlarged lingual tonsil on tongue base was observed and the larynx could not be seen because of large lingual tonsil (B).

Fig. 2. Preoperative contrast-en-hanced CT showed the hypertrophy of lingual tonsil (LT) which markedly obstructed the airway. Axial (A) and sagittal view (B).
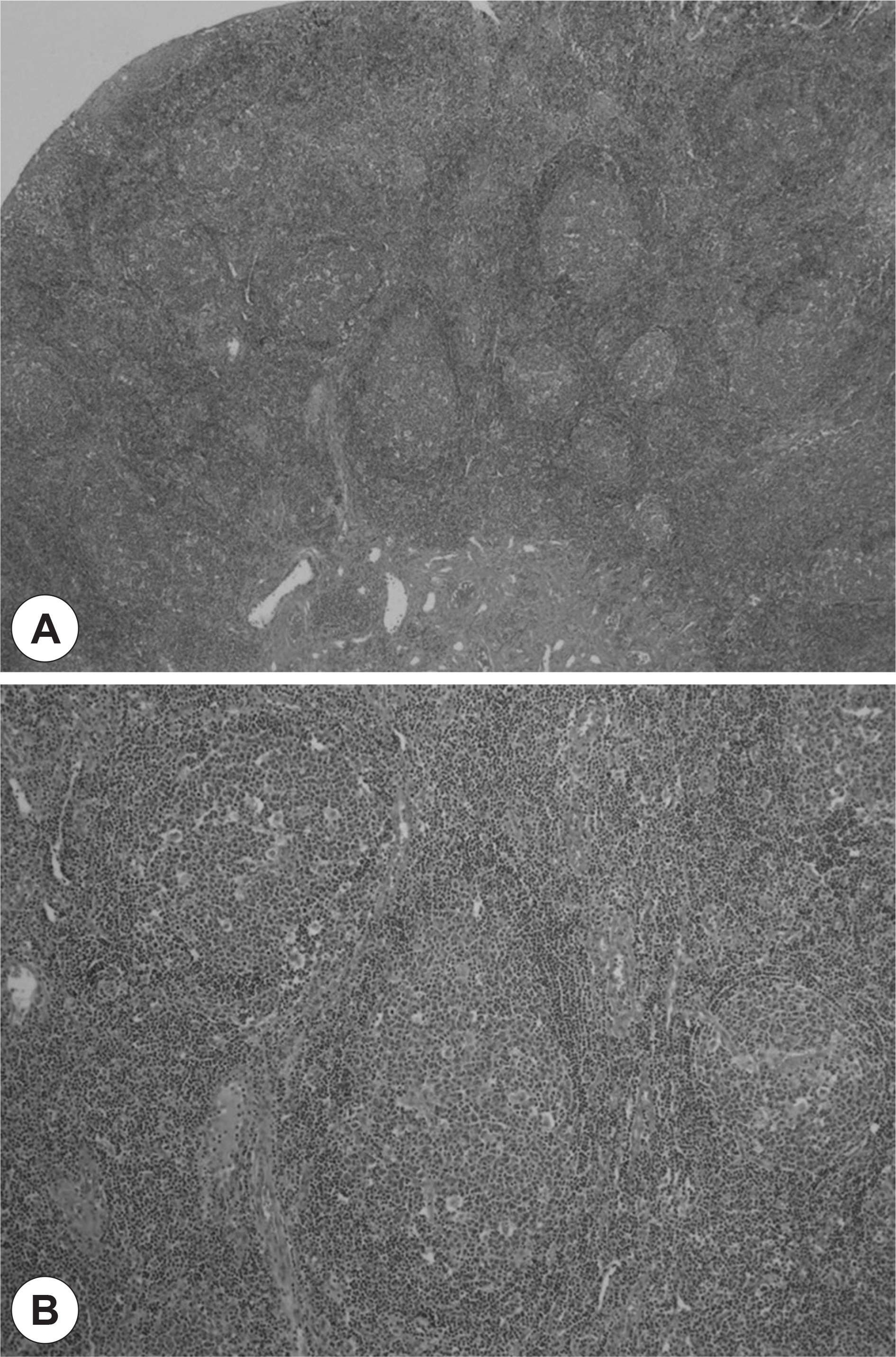
Fig. 3. Pathologic findings. On microscopic view, reactive follicles with normal lymphoid tissue were identified (H&E, ×25) (A). The reactive lymphoid tissue showed excessive increase of the germinal center (H&E, ×50) (B).

Fig. 4. Endoscopic findings (A) and cephalometric lateral radiograph (B) at 5 months after operation. The endoscopic findings showed reduced lingual tonsil and the normal laryngeal column. The cephalometric lateral radiograph showed that the airway is patent.
Reference
-
References
1). Kim J, In K, Kim J, You S, Kang K, Shim J, et al. Prevalence of sleep-disordered breathing in middle-aged Korean men and women. Am J Respir Crit Care Med. 2004; 170(10):1108–13.
Article2). Friedman M, Ibrahim H, Bass L. Clinical staging for sleep-disor-dered breathing. Otolaryngol Head Neck Surg. 2002; 127(1):13–21.
Article3). Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013; 177(9):1006–14.
Article4). Strohl KP, Brown DB, Collop N, George C, Grunstein R, Han F, et al. An official American Thoracic Society Clinical Practice Guideline: sleep apnea, sleepiness, and driving risk in noncommercial drivers. An update of a 1994 Statement. Am J Respir Crit Care Med. 2013; 187(11):1259–66.
Article5). Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000; 342(19):1378–84.
Article6). Breitmeier D, Wilke N, Schulz Y, Albrecht K, Wenzel V, Kleemann WJ, et al. The lingual tonsillar hyperplasia in relation to unantici-pated difficult intubation: is there any relationship between lingual tonsillar hyperplasia and tonsillectomy? Am J Forensic Med Pathol. 2005; 26(2):131–5.7). Robinson S, Ettema SL, Brusky L, Woodson BT. Lingual tonsillectomy using bipolar radiofrequency plasma excision. Otolaryngol Head Neck Surg. 2006; 134(2):328–30.
Article8). Abdel-Aziz M, Ibrahim N, Ahmed A, El-Hamamsy M, Abdel-Kha-lik MI, El-Hoshy H. Lingual tonsils hypertrophy; a cause of obstructive sleep apnea in children after adenotonsillectomy: operative problems and management. Int J Pediatr Otorhinolaryngol. 2011; 75(9):1127–31.
Article9). Acar GÖ. Cansz H, Duman C, Öz B, Ciğercioğullar E. Excessive Reactive Lymphoid Hyperplasia in a Child With Persistent Obstructive Sleep Apnea Despite Previous Tonsillectomy and Adenoidectomy. J Craniofac Surg. 2011; 22(4):1413–5.10). Parham K, Newman R. Recurrent lingual tonsil hyperplasia. Arch Otolaryngol Head Neck Surg. 2003; 129(9):1010–2.
Article11). Park CH, Shim HJ, Kim EJ, Ahn YM. A Case of Treatment in Obstructive Sleep Apnea Syndrome in Children with Lingual Tonsillar Hypertrophy. Korean J Otorhinolaryngol-Head Neck Surg. 2008; 51(6):562–5.12). Dündar A, Ozünlü A, Sahan M, Ozgen F. Lingual tonsil hypertrophy producing obstructive sleep apnea. Laryngoscope. 1996; 106(9 Pt 1):1167–9.
Article13). Han BD, Shin SM, Kim YR, Ye MK, Shin SH. Effect of Gastroesophageal Reflux on the Symptoms and Treatment Result of Obstructive Sleep Apnea Syndrome. J Rhinol. 2012; 19(1):40–4.14). Marcos Ordóñez M, Benito Orejas JI, Blasco Gutiérrez MJ, Morais Pérez D, Ramírez Cano B. Oropharyngeal tuberculosis. Report of case in a lingual tonsil. Acta Otorrinolaringol Esp. 1999; 50(7):575–8.15). Fricke BL, Donnelly LF, Shott SR, Kalra M, Poe SA, Chini BA, et al. Comparison of lingual tonsil size as depicted on MR imaging between children with obstructive sleep apnoea despite previous tonsillectomy and adenoidectomy and normal controls. Pediatr Radiol. 2006; 36(6):518–23.16). Chung YS. Pathogenesis of Obstructive Sleep Apnea. J Rhinol. 2009; 16(2):87–90.17). Smith PL, Gold AR, Meyers DA, Haponik EF, Bleecker ER. Weight loss in mildly to moderately obese patients with obstructive sleep apnea. Ann Intern Med. 1985; 103(6):850–5.
Article18). Rowley JA, Permutt S, Willey S, Smith PL, Schwartz AR. Effect of tracheal and tongue displacement on upper airway airflow dynamics. J Appl Physiol. 1996; 80(6):2171–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Treatment in Obstructive Sleep Apnea Syndrome in Children with Lingual Tonsillar Hypertrophy
- A Case of Children Suspected as Obstructive Sleep Apnea due to Tubal Tonsillar Hypertrophy
- A Case of Tonsillectomy and Adenoidectomy in Child With Down Syndrome With Obstructive Sleep Apnea
- A Case of Childhood Obstructive Sleep Apnea Syndrome
- Effects of Menopause on Obstructive Sleep Apnea
