J Korean Med Sci.
2015 Apr;30(4):489-494. 10.3346/jkms.2015.30.4.489.
Perioperative Complications of Orthopedic Surgery for Lower Extremity in Patients with Cerebral Palsy
- Affiliations
-
- 1Department of Orthopedic Surgery, Ewha Womans University Mokdong Hospital, Seoul, Korea.
- 2Department of Anesthesiology and Pain Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
- 3Department of Orthopedic Surgery, Seoul National University Bundang Hospital, Seongnam, Korea. pmsmed@gmail.com
- 4Biomedical Research Institute, Seoul National University Bundang Hospital, Seongnam, Korea.
- 5Department of Orthopedic Surgery, Myongji Hospital, Goyang, Korea.
- KMID: 2164459
- DOI: http://doi.org/10.3346/jkms.2015.30.4.489
Abstract
- Because complications are more common in patients with cerebral palsy (CP), surgeons and anesthesiologists must be aware of perioperative morbidity and be prepared to recognize and treat perioperative complications. This study aimed to determine the incidence of and risk factors for perioperative complications of orthopedic surgery on the lower extremities in patients with CP. We reviewed the medical records of consecutive CP patients undergoing orthopedic surgery. Medical history, anesthesia emergence time, intraoperative body temperature, heart rate, blood pressure, immediate postoperative complications, Gross Motor Function Classification System (GMFCS) level, Cormack-Lehane classification, and American Society of Anesthesiologists physical status classification were analyzed. A total of 868 patients was included. Mean age at first surgery was 11.8 (7.6) yr. The incidences of intraoperative hypothermia, absolute hypotension, and absolute bradycardia were 26.2%, 4.4%, and 20.0%, respectively. Twenty (2.3%) patients had major complications, and 35 (4.0%) patients had minor complications postoperatively. The incidences of intraoperative hypothermia, absolute hypotension, and major postoperative complications were significantly higher in patients at GMFCS levels IV and V compared with patients at GMFCS levels I to III (P<0.001). History of pneumonia was associated with intraoperative absolute hypotension and major postoperative complications (P<0.001). These results revealed that GMFCS level, patient age, hip reconstructive surgery, and history of pneumonia are associated with adverse effects on intraoperative body temperature, the cardiovascular system, and immediate postoperative complications.
Keyword
MeSH Terms
Figure
-
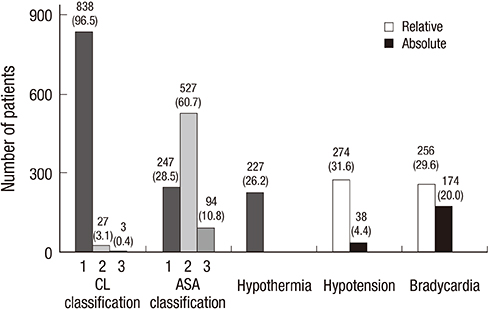
Fig. 1 Patient distribution according to CL classification and ASA classification levels and overall incidence of intraoperative hypothermia, hypotension, and bradycardia (Number of patients [%]; CL, Cormack and Lehane; ASA class, American Society of Anesthesiologist Physical Status Classification System).
Reference
-
1. Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Damiano D, Dan B, Jacobsson B. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007; 109:8–14.2. Wongprasartsuk P, Stevens J. Cerebral palsy and anaesthesia. Paediatr Anaesth. 2002; 12:296–303.3. Baxter P. Comorbidities of cerebral palsy need more emphasis--especially pain. Dev Med Child Neurol. 2013; 55:396.4. Woo SJ, Ahn J, Park MS, Lee KM, Gwon DK, Hwang JM, Chung CY. Ocular findings in cerebral palsy patients undergoing orthopedic surgery. Optom Vis Sci. 2011; 88:1520–1523.5. Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997; 39:214–223.6. Sung KH, Chung CY, Lee KM, Akhmedov B, Lee SY, Choi IH, Cho TJ, Yoo WJ, Park MS. Long term outcome of single event multilevel surgery in spastic diplegia with flexed knee gait. Gait Posture. 2013; 37:536–541.7. Park MS, Chung CY, Kwon DG, Sung KH, Choi IH, Lee KM. Prophylactic femoral varization osteotomy for contralateral stable hips in non-ambulant individuals with cerebral palsy undergoing hip surgery: decision analysis. Dev Med Child Neurol. 2012; 54:231–239.8. Park MS, Chung CY, Lee SH, Cho TJ, Yoo WJ, Choi IH. Two-dimensional computed tomographic measurement of acetabulum--reliability, validity, and limitation. J Pediatr Orthop. 2008; 28:812–818.9. Master DL, Son-Hing JP, Poe-Kochert C, Armstrong DG, Thompson GH. Risk factors for major complications after surgery for neuromuscular scoliosis. Spine (Phila Pa 1976). 2011; 36:564–571.10. Shore BJ, White N, Kerr Graham H. Surgical correction of equinus deformity in children with cerebral palsy: a systematic review. J Child Orthop. 2010; 4:277–290.11. Tis JE, Sharif S, Shannon B, Dabney K, Miller F. Complications associated with multiple, sequential osteotomies for children with cerebral palsy. J Pediatr Orthop B. 2006; 15:408–413.12. Wass CT, Warner ME, Worrell GA, Castagno JA, Howe M, Kerber KA, Palzkill JM, Schroeder DR, Cascino GD. Effect of general anesthesia in patients with cerebral palsy at the turn of the new millennium: a population-based study evaluating perioperative outcome and brief overview of anesthetic implications of this coexisting disease. J Child Neurol. 2012; 27:859–866.13. Ranstam J. Repeated measurements, bilateral observations and pseudoreplicates, why does it matter? Osteoarthritis Cartilage. 2012; 20:473–475.14. McGinley JL, Dobson F, Ganeshalingam R, Shore BJ, Rutz E, Graham HK. Single-event multilevel surgery for children with cerebral palsy: a systematic review. Dev Med Child Neurol. 2012; 54:117–128.15. Spencer JD. Reconstruction of dislocated hips in children with cerebral palsy. BMJ. 1999; 318:1021–1022.16. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia. 1984; 39:1105–1111.17. Dripps RD, Lamont A, Eckenhoff JE. The role of anesthesia in surgical mortality. JAMA. 1961; 178:261–266.18. Krage R, van Rijn C, van Groeningen D, Loer SA, Schwarte LA, Schober P. Cormack-Lehane classification revisited. Br J Anaesth. 2010; 105:220–227.19. Aplin S, Baines D, DE Lima J. Use of the ASA Physical Status Grading System in pediatric practice. Paediatr Anaesth. 2007; 17:216–222.20. Kurz A, Sessler DI, Lenhardt R. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization. Study of Wound Infection and Temperature Group. N Engl J Med. 1996; 334:1209–1215.21. Lenhardt R, Marker E, Goll V, Tschernich H, Kurz A, Sessler DI, Narzt E, Lackner F. Mild intraoperative hypothermia prolongs postanesthetic recovery. Anesthesiology. 1997; 87:1318–1323.22. Nafiu OO, Voepel-Lewis T, Morris M, Chimbira WT, Malviya S, Reynolds PI, Tremper KK. How do pediatric anesthesiologists define intraoperative hypotension? Paediatr Anaesth. 2009; 19:1048–1053.23. Kraemer FW, Stricker PA, Gurnaney HG, McClung H, Meador MR, Sussman E, Burgess BJ, Ciampa B, Mendelsohn J, Rehman MA, et al. Bradycardia during induction of anesthesia with sevoflurane in children with Down syndrome. Anesth Analg. 2010; 111:1259–1263.24. Clardy CW, Edwards KM, Gay JC. Increased susceptibility to infection in hypothermic children: possible role of acquired neutrophil dysfunction. Pediatr Infect Dis. 1985; 4:379–382.25. Horosz B, Malec-Milewska M. Inadvertent intraoperative hypothermia. Anaesthesiol Intensive Ther. 2013; 45:38–43.26. Kalezic N, Stojanovic M, Ladjevic N, Markovic D, Paunovic I, Palibrk I, Milicic B, Sabljak V, Antonijevic V, Ivanovic B, et al. Risk factors for intraoperative hypotension during thyroid surgery. Med Sci Monit. 2013; 19:236–241.27. Reich DL, Hossain S, Krol M, Baez B, Patel P, Bernstein A, Bodian CA. Predictors of hypotension after induction of general anesthesia. Anesth Analg. 2005; 101:622–628.28. Stasikelis PJ, Lee DD, Sullivan CM. Complications of osteotomies in severe cerebral palsy. J Pediatr Orthop. 1999; 19:207–210.29. Verschuren O, Takken T. Aerobic capacity in children and adolescents with cerebral palsy. Res Dev Disabil. 2010; 31:1352–1357.30. Lundberg A. Maximal aerobic capacity of young people with spastic cerebral palsy. Dev Med Child Neurol. 1978; 20:205–210.31. Park MS, Chung CY, Lee KM, Lee SH, Choi IH, Cho TJ, Yoo WJ, Kim KH. Issues of concern before single event multilevel surgery in patients with cerebral palsy. J Pediatr Orthop. 2010; 30:489–495.32. Hightower CE, Riedel BJ, Feig BW, Morris GS, Ensor JE Jr, Woodruff VD, Daley-Norman MD, Sun XG. A pilot study evaluating predictors of postoperative outcomes after major abdominal surgery: physiological capacity compared with the ASA physical status classification system. Br J Anaesth. 2010; 104:465–471.33. Fu KM, Smith JS, Polly DW Jr, Ames CP, Berven SH, Perra JH, McCarthy RE, Knapp DR Jr, Shaffrey CI. Scoliosis Research Society Morbidity and Mortality Committee. Correlation of higher preoperative American Society of Anesthesiology grade and increased morbidity and mortality rates in patients undergoing spine surgery. J Neurosurg Spine. 2011; 14:470–474.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- End Results of Operative Treatment on 18 Cases 40 procdures of Cerebral Palsy
- Surgical Strategies and Perioperative Considerations for Cervical Deformity With Cerebral Palsy: A Comprehensive Review of the Literature
- Current opinion of cerebral palsy
- The Effects of Single Event Multi-level Chemoneurolysis on Upper Extremity Function in Children with Cerebral Palsy
- Anterior Knee Pain in Patients with Cerebral Palsy
