Yonsei Med J.
2015 Sep;56(5):1421-1427. 10.3349/ymj.2015.56.5.1421.
Effects of Alveolar Recruitment and Positive End-Expiratory Pressure on Oxygenation during One-Lung Ventilation in the Supine Position
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. yjoh@yuhs.ac
- 2Department of Thoracic and Cardiovascular Surgery, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- KMID: 2163639
- DOI: http://doi.org/10.3349/ymj.2015.56.5.1421
Abstract
- PURPOSE
Hypoxemia during one-lung ventilation (OLV) remains a serious problem, particularly in the supine position. We investigated the effects of alveolar recruitment (AR) and positive end-expiratory pressure (PEEP) on oxygenation during OLV in the supine position.
MATERIALS AND METHODS
Ninety-nine patients were randomly allocated to one of the following three groups: a control group (ventilation with a tidal volume of 8 mL/kg), a PEEP group (the same ventilatory pattern with a PEEP of 8 cm H2O), or an AR group (an AR maneuver immediately before OLV followed by a PEEP of 8 cm H2O). The tidal volume was reduced to 6 mL/kg during OLV in all groups. Blood gas analyses, respiratory variables, and hemodynamic variables were recorded 15 min into TLV (TLVbaseline), 15 and 30 min after OLV (OLV15 and OLV30), and 10 min after re-establishing TLV (TLVend).
RESULTS
Ultimately, 92 patients were analyzed. In the AR group, the arterial oxygen tension was higher at TLVend, and the physiologic dead space was lower at OLV15 and TLVend than in the control group. The mean airway pressure and dynamic lung compliance were higher in the PEEP and AR groups than in the control group at OLV15, OLV30, and TLVend. No significant differences in hemodynamic variables were found among the three groups throughout the study period.
CONCLUSION
Recruitment of both lungs with subsequent PEEP before OLV improved arterial oxygenation and ventilatory efficiency during video-assisted thoracic surgery requiring OLV in the supine position.
Keyword
MeSH Terms
-
Adult
Aged
Anoxia
Female
Humans
Lung/physiopathology
Lung Compliance/physiology
Male
Middle Aged
One-Lung Ventilation/*methods
Oxygen/*blood
Positive-Pressure Respiration/*methods
Pulmonary Alveoli/*physiology
Pulmonary Gas Exchange
Respiratory Mechanics/*physiology
*Supine Position
Thoracic Surgery, Video-Assisted
Tidal Volume
Oxygen
Figure
-
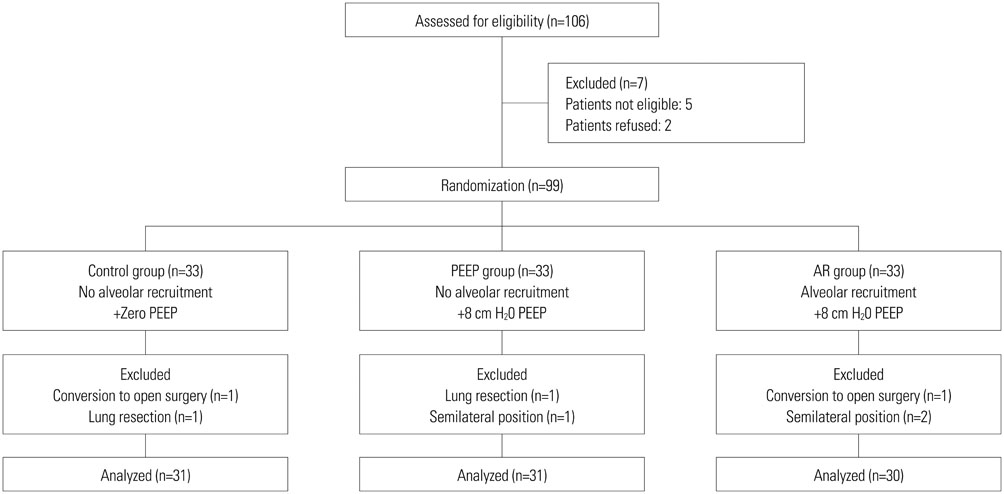
Fig. 1 The consort flow diagram. PEEP, positive end-expiratory pressure.
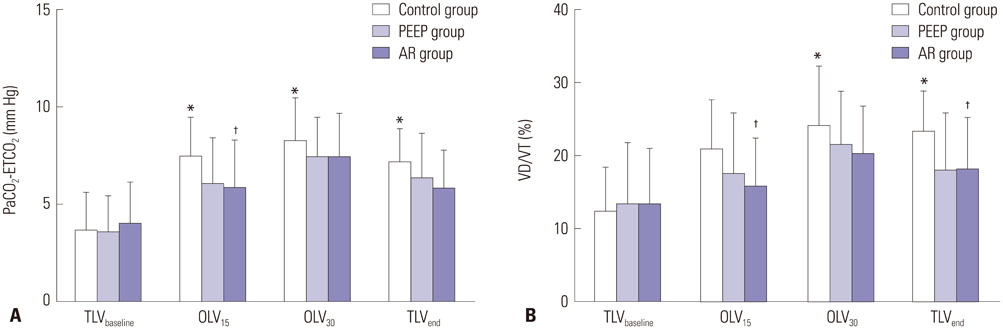
Fig. 2 Changes in the PaCO2-ETCO2 difference (A) and estimated VD/VT (B). PaCO2-ETCO2, arterial to end-tidal carbon dioxide tension difference; estimated VD/VT, physiologic dead space. *p<0.05 vs. TLVbaseline in each group, †p<0.05 vs. control group.
Reference
-
1. Darlong LM. Video-assisted thoracic surgery for superior posterior mediastinal neurogenic tumour in the supine position. J Minim Access Surg. 2009; 5:49–51.
Article2. Nesher N, Pevni D, Aviram G, Kramer A, Mohr R, Uretzky G, et al. Video-assisted thymectomy with contralateral surveillance camera: a means to minimize the risk of contralateral phrenic nerve injury. Innovations (Phila). 2012; 7:266–269.
Article3. Jurado J, Javidfar J, Newmark A, Lavelle M, Bacchetta M, Gorenstein L, et al. Minimally invasive thymectomy and open thymectomy: outcome analysis of 263 patients. Ann Thorac Surg. 2012; 94:974–981.
Article4. Watanabe S, Noguchi E, Yamada S, Hamada N, Kano T. Sequential changes of arterial oxygen tension in the supine position during one-lung ventilation. Anesth Analg. 2000; 90:28–34.5. Nyrén S, Radell P, Lindahl SG, Mure M, Petersson J, Larsson SA, et al. Lung ventilation and perfusion in prone and supine postures with reference to anesthetized and mechanically ventilated healthy volunteers. Anesthesiology. 2010; 112:682–687.
Article6. Bardoczky GI, Szegedi LL, d'Hollander AA, Moures JM, de Francquen P, Yernault JC. Two-lung and one-lung ventilation in patients with chronic obstructive pulmonary disease: the effects of position and F(IO)2. Anesth Analg. 2000; 90:35–41.
Article7. Hedenstierna G, Tenling A. The lung during and after thoracic anaesthesia. Curr Opin Anaesthesiol. 2005; 18:23–28.
Article8. Hedenstierna G, Tokics L, Strandberg A, Lundquist H, Brismar B. Correlation of gas exchange impairment to development of atelectasis during anaesthesia and muscle paralysis. Acta Anaesthesiol Scand. 1986; 30:183–191.
Article9. Strandberg A, Tokics L, Brismar B, Lundquist H, Hedenstierna G. Atelectasis during anaesthesia and in the postoperative period. Acta Anaesthesiol Scand. 1986; 30:154–158.
Article10. Unzueta C, Tusman G, Suarez-Sipmann F, Böhm S, Moral V. Alveolar recruitment improves ventilation during thoracic surgery: a randomized controlled trial. Br J Anaesth. 2012; 108:517–524.
Article11. Park SH, Jeon YT, Hwang JW, Do SH, Kim JH, Park HP. A preemptive alveolar recruitment strategy before one-lung ventilation improves arterial oxygenation in patients undergoing thoracic surgery: a prospective randomised study. Eur J Anaesthesiol. 2011; 28:298–302.
Article12. Tusman G, Böhm SH, Sipmann FS, Maisch S. Lung recruitment improves the efficiency of ventilation and gas exchange during one-lung ventilation anesthesia. Anesth Analg. 2004; 98:1604–1609.
Article13. Tusman G, Böhm SH, Melkun F, Staltari D, Quinzio C, Nador C, et al. Alveolar recruitment strategy increases arterial oxygenation during one-lung ventilation. Ann Thorac Surg. 2002; 73:1204–1209.
Article14. Valenza F, Ronzoni G, Perrone L, Valsecchi M, Sibilla S, Nosotti M, et al. Positive end-expiratory pressure applied to the dependent lung during one-lung ventilation improves oxygenation and respiratory mechanics in patients with high FEV1. Eur J Anaesthesiol. 2004; 21:938–943.
Article15. Hoftman N, Canales C, Leduc M, Mahajan A. Positive end expiratory pressure during one-lung ventilation: selecting ideal patients and ventilator settings with the aim of improving arterial oxygenation. Ann Card Anaesth. 2011; 14:183–187.
Article16. Inomata S, Nishikawa T, Saito S, Kihara S. "Best" PEEP during one-lung ventilation. Br J Anaesth. 1997; 78:754–756.17. Rozé H, Lafargue M, Perez P, Tafer N, Batoz H, Germain C, et al. Reducing tidal volume and increasing positive end-expiratory pressure with constant plateau pressure during one-lung ventilation: effect on oxygenation. Br J Anaesth. 2012; 108:1022–1027.18. Czepizak CA, O'Callaghan JM, Venus B. Evaluation of formulas for optimal positioning of central venous catheters. Chest. 1995; 107:1662–1664.19. Hardman JG, Aitkenhead AR. Estimating alveolar dead space from the arterial to end-tidal CO(2) gradient: a modeling analysis. Anesth Analg. 2003; 97:1846–1851.
Article20. De Giacomo T, Diso D, Anile M, Venuta F, Rolla M, Ricella C, et al. Thoracoscopic resection of mediastinal bronchogenic cysts in adults. Eur J Cardiothorac Surg. 2009; 36:357–359.21. Meyer DM, Herbert MA, Sobhani NC, Tavakolian P, Duncan A, Bruns M, et al. Comparative clinical outcomes of thymectomy for myasthenia gravis performed by extended transsternal and minimally invasive approaches. Ann Thorac Surg. 2009; 87:385–390.
Article22. Karzai W, Schwarzkopf K. Hypoxemia during one-lung ventilation: prediction, prevention, and treatment. Anesthesiology. 2009; 110:1402–1411.23. Tang L, Kazan R, Taddei R, Zaouter C, Cyr S, Hemmerling TM. Reduced cerebral oxygen saturation during thoracic surgery predicts early postoperative cognitive dysfunction. Br J Anaesth. 2012; 108:623–629.24. Hedenstierna G, Sandhagen B. Assessing dead space. A meaningful variable? Minerva Anestesiol. 2006; 72:521–528.25. Fletcher R. The arterial-end-tidal CO2 difference during cardiothoracic surgery. J Cardiothorac Anesth. 1990; 4:105–117.26. Sentürk NM, Dilek A, Camci E, Sentürk E, Orhan M, Tugğrul M, et al. Effects of positive end-expiratory pressure on ventilatory and oxygenation parameters during pressure-controlled one-lung ventilation. J Cardiothorac Vasc Anesth. 2005; 19:71–75.27. Kehlet H, Holte K. Effect of postoperative analgesia on surgical outcome. Br J Anaesth. 2001; 87:62–72.28. Youssef SJ, Louie BE, Farivar AS, Blitz M, Aye RW, Vallières E. Comparison of open and minimally invasive thymectomies at a single institution. Am J Surg. 2010; 199:589–593.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effects of Repetitive Alveolar Recruitment on Oxygenation and Compliance in ARDS Patients
- Effect of High Frequency Jet Ventilation alone or with Positive End Expiratory Pressure on the Arterial Oxygenation during One Lung Ventilation
- Effect of Recruiting Maneuvers in a Patient with Acute Lung Injury after Femoral Nailing: A case report
- Ventilator-Induced Lung Injury
- Effects of a preemptive alveolar recruitment strategy on arterial oxygenation during one-lung ventilation with different tidal volumes in patients with normal pulmonary function test
