Subperiosteal Osteoid Osteoma of the Knee: Case Report
- Affiliations
-
- 1Department of Radiology, Pusan National University Hospital, Biomedical Research Institute, Busan, Korea. lis@pusan.ac.kr
- 2Pusan National University School of Medicine, Busan, Korea.
- 3Department of Orthopaedic Surgery, Pusan National University Hospital, Biomedical Research Institute, Busan, Korea.
- 4Department of Radiology, Inje University Haeundae Paik Hospital, Busan, Korea.
- KMID: 2161371
- DOI: http://doi.org/10.13104/imri.2016.20.1.61
Abstract
- Osteoid osteoma, a frequent lesions of bone, is usually intraosseous but occasionally subperiosteal. We describe the case of a 19-year-old male with knee pain caused by subperiosteal osteoid osteoma. Radiologic evaluation was performed with radiographic, computed tomography (CT), ultrasonographic (US) and magnetic resonance imaging (MRI). But the preoperative diagnosis of osteoid osteoma was delayed because of unusual imaging findings and atypical symptom. After excisional biopsy, histological examination confirmed the diagnosis of osteoid osteoma. The lesion was treated successfully with CT-guided radiofrequency ablation.
Keyword
MeSH Terms
Figure
-
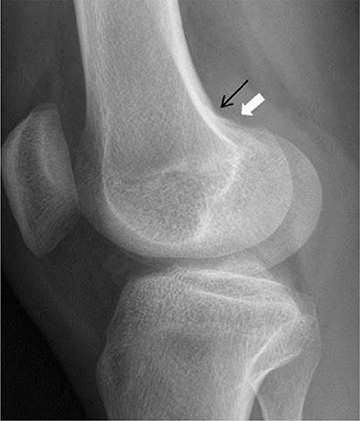
Fig. 1 Radiograph of the right knee taken at initial visit showed faint mineralization (white arrow) adjacent to the superior cortex of the lateral femoral condyle with focal, smooth erosion of cortex (black arrow) at the distal femur.
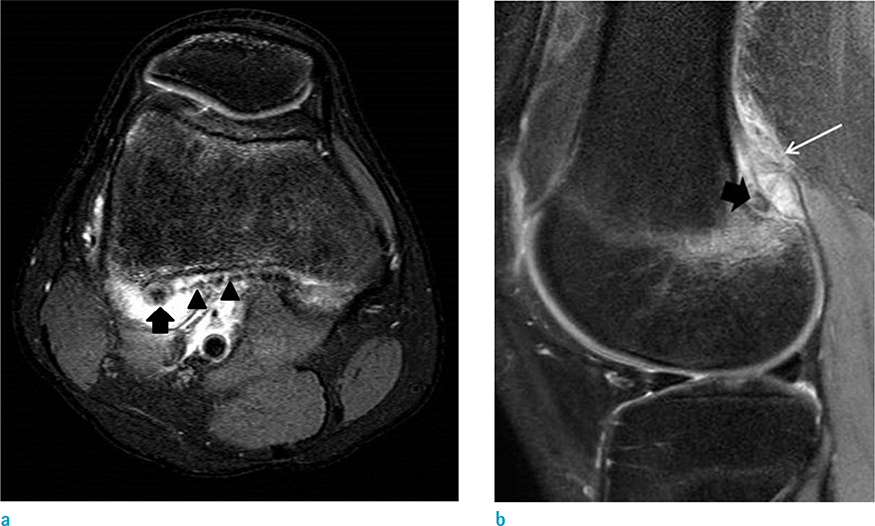
Fig. 2 MR images of the right knee obtained 7 days after plain radiography. (a) Axial fat-suppressed T2-weighted and (b) sagittal fat-suppressed proton-density images show extensive bone marrow and soft tissue edema (white arrows) in the lateral femoral condyle. A small, round nodular lesion of low signal intensity (black arrows) was visualized at the extracortical and subperiosteal area adjacent to the insertion site of the lateral head of the gastrocnemius muscle. Also elevated periosteum (black arrowheads) was noted, so the lesion was thought to be in subperiosteal area.
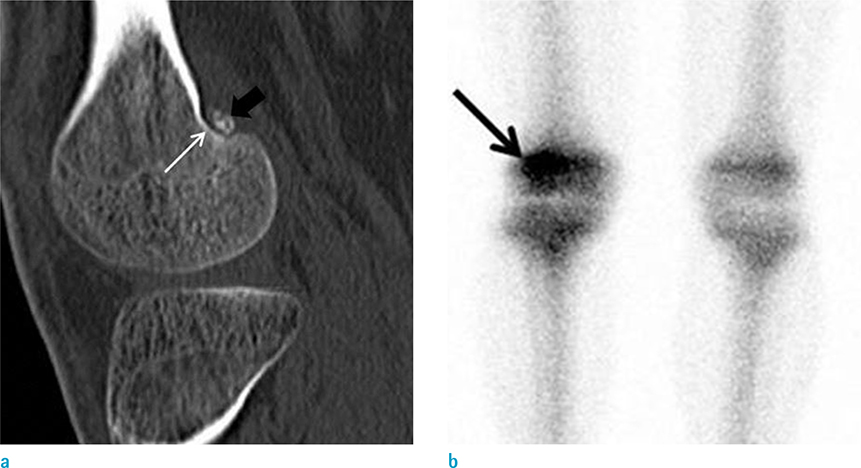
Fig. 3 (a) CT scan shows the small nodular lesion with calcification (black arrow) located in the subperiosteal area causing smooth erosion of adjacent cortex (white arrow). (b) Bone scan shows increased uptake of isotope (arrow) at the right lateral femoral condyle.
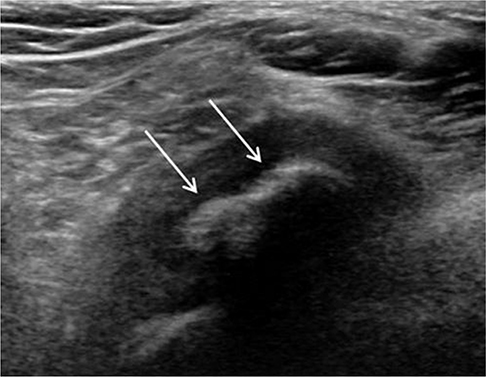
Fig. 4 Axial ultrasonogram taken before needling showing a hyperechoic lesion with a lobulated contour and posterior shadowing, representing calcification (arrows) in the posterolateral aspect of right knee.

Fig. 5 Grossly, the resected specimen appeared as a firm, lobulated, red-colored mass of diameter 0.5 cm.
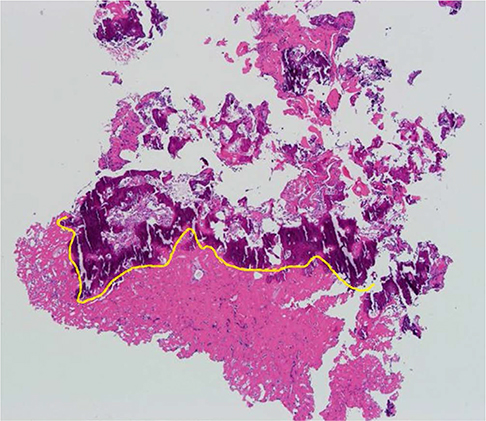
Fig. 6 Microscopically (× 40), the lesion was composed of anastomosing trabeculae of woven bone (above the yellow line, around the nidus) and a solid, sclerotic nidus (below the yellow line).
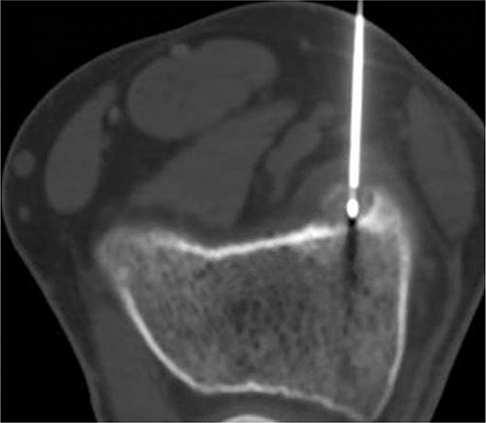
Fig. 7 Curative treatment was undertaken by radio-frequency ablation (RFA). RFA needle was well located in the center of the nidus.
Reference
-
1. Suresh SS, Rani V. Atypical periosteal osteoid osteoma: a case report. Cases J. 2009; 2:124.2. Kayser F, Resnick D, Haghighi P, et al. Evidence of the subperiosteal origin of osteoid osteomas in tubular bones: analysis by CT and MR imaging. AJR Am J Roentgenol. 1998; 170:609–614.3. Khan JA, Vaidya S, Devkota P, Acharya BM, Pradhan NM, Shrestha S. Subperiosteal osteoid osteoma of the neck of talus. JNMA J Nepal Med Assoc. 2009; 48:58–61.4. Kitsoulis P, Mantellos G, Vlychou M. Osteoid osteoma. Acta Orthop Belg. 2006; 72:119–125.5. Motamedi D, Learch TJ, Ishimitsu DN, et al. Thermal ablation of osteoid osteoma: overview and step-by-step guide. Radiographics. 2009; 29:2127–2141.6. Cakar M, Esenyel CZ, Seyran M, et al. Osteoid osteoma treated with radiofrequency ablation. Adv Orthop. 2015; 2015:807274.7. Chai JW, Hong SH, Choi JY, et al. Radiologic diagnosis of osteoid osteoma: from simple to challenging findings. Radiographics. 2010; 30:737–749.
