Yonsei Med J.
2013 Jul;54(4):957-964. 10.3349/ymj.2013.54.4.957.
Preventive Effect of Pretreatment with Intravenous Nicorandil on Contrast-Induced Nephropathy in Patients with Renal Dysfunction Undergoing Coronary Angiography (PRINCIPLE Study)
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.
- 2Division of Cardiology, Gangam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. cardiobk@yuhs.ac
- 3Division of Cardiology, Gil Medical Center, Incheon, Korea.
- 4Division of Cardiology, Bundang Cha Hospital, Seongnam, Korea.
- 5Division of Cardiology, Myongji Hospital, Goyang, Korea.
- 6Division of Cardiology, Kangnam Sacred Heart Hospital, Seoul, Korea.
- KMID: 2158232
- DOI: http://doi.org/10.3349/ymj.2013.54.4.957
Abstract
- PURPOSE
To investigate the effect of pretreatment with intravenous nicorandil on the incidence of contrast-induced nephropathy (CIN) in patients with renal dysfunction undergoing coronary angiography.
MATERIALS AND METHODS
This randomized controlled multicenter study enrolled a total of 166 patients (nicorandil n=81; control n=85) with an estimated glomerular filtration rate <60 mL/min. Nicorandil 12 mg dissolved in 100 mL of 0.9% saline was administered intravenously for 30 minutes just prior to coronary angiography in the nicorandil group. The same volume of only saline was given to the control group. The primary end-point was the incidence of CIN, defined as >0.5 mg/dL increase or >25% rise in serum creatinine (SCr) concentration within 48 hours of contrast exposure compared to baseline.
RESULTS
The final analysis included 149 patients (nicorandil n=73; control n=76). The baseline characteristics and the total volume of the used contrast (Iodixanol, 125.6+/-69.1 mL vs. 126.9+/-74.6 mL, p=0.916) were similar between the two groups. The incidence of CIN also did not differ between the nicorandil and control groups (6.8% vs. 6.6%, p=0.794). There was no difference between the two groups in the relative change in SCr from baseline to peak level within 48 hours after coronary angiography (-1.58+/-24.07% vs. 0.96+/-17.49%, p=0.464), although the nicorandil group showed less absolute change in SCr than the control group (-0.01+/-0.43 mg/mL vs. 0.02+/-0.31 mg/mL, p=0.005).
CONCLUSION
Prophylactic intravenous infusion of nicorandil did not decrease the incidence of CIN in patients with renal dysfunction undergoing coronary angiography.
MeSH Terms
-
Administration, Intravenous
Aged
Contrast Media/*adverse effects
Coronary Angiography/*adverse effects/methods
Creatinine/blood
Female
Glomerular Filtration Rate
Humans
Incidence
Kidney Diseases/*chemically induced/epidemiology/physiopathology/*prevention & control
Male
Middle Aged
Nicorandil/*administration & dosage/therapeutic use
Contrast Media
Nicorandil
Creatinine
Figure
-
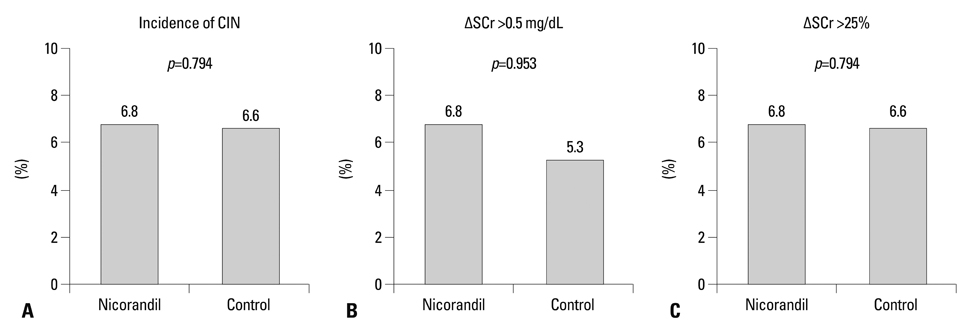
Fig. 1 Changes in serum creatinine levels. (A) Incidence of contrast-induced nephropathy. (B) Frequency of an increase in serum creatinine level >0.5 mg/dL from baseline. (C) Frequency of an increase in serum creatinine level >25% from baseline. CIN, contrast-induced nephropathy; SCr, serum creatinine.
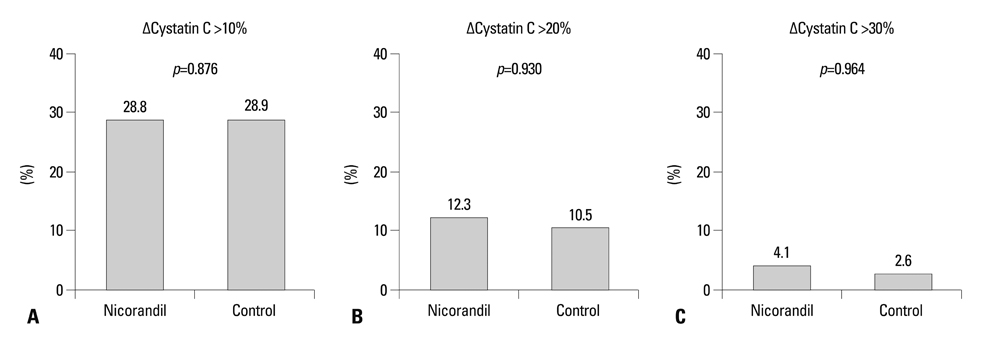
Fig. 2 Changes in serum cystatin C levels. Frequency of increases in serum cystatin C >10% (A), >20% (B), and >30% (C) from baseline.
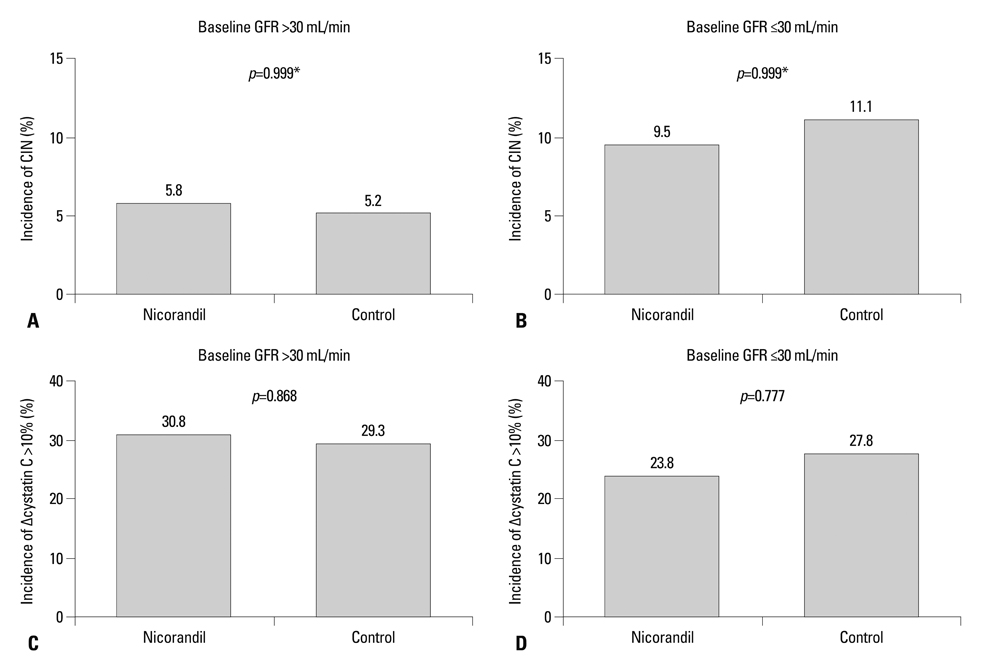
Fig. 3 Incidences of CIN (A and C) and increase in serum cystatin C >10% from baseline (B and D) in patient subgroups with baseline glomerular filtration rate (GFR) >30 mL/min (A and B) and ≤30 mL/min (C and D). *p value by Fisher exact test. CIN, contrast-induced nephropathy.
Reference
-
1. McCullough PA, Wolyn R, Rocher LL, Levin RN, O'Neill WW. Acute renal failure after coronary intervention: incidence, risk factors, and relationship to mortality. Am J Med. 1997; 103:368–375.2. Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002; 39:930–936.
Article3. Kim MJ, Choi HS, Oh SH, Lee HC, Kim CS, Choi JS, et al. Impact of acute kidney injury on clinical outcomes after ST elevation acute myocardial infarction. Yonsei Med J. 2011; 52:603–609.
Article4. Rihal CS, Textor SC, Grill DE, Berger PB, Ting HH, Best PJ, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002; 105:2259–2264.
Article5. Mehran R, Aymong ED, Nikolsky E, Lasic Z, Iakovou I, Fahy M, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004; 44:1393–1399.
Article6. Persson PB, Hansell P, Liss P. Pathophysiology of contrast medium-induced nephropathy. Kidney Int. 2005; 68:14–22.
Article7. Wong PC, Li Z, Guo J, Zhang A. Pathophysiology of contrast-induced nephropathy. Int J Cardiol. 2012; 158:186–192.
Article8. Taira N. Nicorandil as a hybrid between nitrates and potassium channel activators. Am J Cardiol. 1989; 63:18J–24J.
Article9. Sun Z, Zhang X, Ito K, Li Y, Montgomery RA, Tachibana S, et al. Amelioration of oxidative mitochondrial DNA damage and deletion after renal ischemic injury by the KATP channel opener diazoxide. Am J Physiol Renal Physiol. 2008; 294:F491–F498.10. Dangas G, Iakovou I, Nikolsky E, Aymong ED, Mintz GS, Kipshidze NN, et al. Contrast-induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables. Am J Cardiol. 2005; 95:13–19.
Article11. Brezis M, Heyman SN, Dinour D, Epstein FH, Rosen S. Role of nitric oxide in renal medullary oxygenation. Studies in isolated and intact rat kidneys. J Clin Invest. 1991; 88:390–395.
Article12. Brenner BM, Troy JL, Ballermann BJ. Endothelium-dependent vascular responses. Mediators and mechanisms. J Clin Invest. 1989; 84:1373–1378.
Article13. Myers SI, Wang L, Liu F, Bartula LL. Iodinated contrast induced renal vasoconstriction is due in part to the downregulation of renal cortical and medullary nitric oxide synthesis. J Vasc Surg. 2006; 44:383–391.
Article14. Fujisaki K, Kubo M, Masuda K, Tokumoto M, Hirakawa M, Ikeda H, et al. Infusion of radiocontrast agents induces exaggerated release of urinary endothelin in patients with impaired renal function. Clin Exp Nephrol. 2003; 7:279–283.
Article15. Ellis JH, Cohan RH. Reducing the risk of contrast-induced nephropathy: a perspective on the controversies. AJR Am J Roentgenol. 2009; 192:1544–1549.
Article16. Spargias K, Adreanides E, Demerouti E, Gkouziouta A, Manginas A, Pavlides G, et al. Iloprost prevents contrast-induced nephropathy in patients with renal dysfunction undergoing coronary angiography or intervention. Circulation. 2009; 120:1793–1799.
Article17. Onbasili AO, Yeniceriglu Y, Agaoglu P, Karul A, Tekten T, Akar H, et al. Trimetazidine in the prevention of contrast-induced nephropathy after coronary procedures. Heart. 2007; 93:698–702.
Article18. Quayle JM, Nelson MT, Standen NB. ATP-sensitive and inwardly rectifying potassium channels in smooth muscle. Physiol Rev. 1997; 77:1165–1232.
Article19. Miki T, Seino S. Roles of KATP channels as metabolic sensors in acute metabolic changes. J Mol Cell Cardiol. 2005; 38:917–925.20. Sato T, Sasaki N, O'Rourke B, Marbán E. Nicorandil, a potent cardioprotective agent, acts by opening mitochondrial ATP-dependent potassium channels. J Am Coll Cardiol. 2000; 35:514–518.
Article21. Shimizu S, Saito M, Kinoshita Y, Ohmasa F, Dimitriadis F, Shomori K, et al. Nicorandil ameliorates ischaemia-reperfusion injury in the rat kidney. Br J Pharmacol. 2011; 163:272–282.
Article22. Lee TM, Chang NC. Effect of nicorandil on proteinuria in well controlled hypertensive patients. J Hypertens. 2009; 27:618–625.
Article23. Ishii H, Ichimiya S, Kanashiro M, Amano T, Imai K, Murohara T, et al. Impact of a single intravenous administration of nicorandil before reperfusion in patients with ST-segment-elevation myocardial infarction. Circulation. 2005; 112:1284–1288.
Article24. Molitoris BA, Levin A, Warnock DG, Joannidis M, Mehta RL, Kellum JA, et al. Improving outcomes of acute kidney injury: report of an initiative. Nat Clin Pract Nephrol. 2007; 3:439–442.
Article25. Solomon R, Dauerman HL. Contrast-induced acute kidney injury. Circulation. 2010; 122:2451–2455.
Article26. Briguori C, Visconti G, Rivera NV, Focaccio A, Golia B, Giannone R, et al. Cystatin C and contrast-induced acute kidney injury. Circulation. 2010; 121:2117–2122.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of N-Acetylcysteine in Prevention of Contrast-Induced Nephropathy after Coronary Angiography
- Contrast-induced Nephropathy in Patients Undergoing Percutaneous Coronary Angiography and its Clinical Characteristics
- A Case of Successful Recovery from High Dose Intravenous Nicorandil Infusion in Refractory Coronary Vasospasm with Hemodynamic Collapse
- N-acetylcysteine for Prevention of Contrast-Induced Nephropathy: A Narrative Review
- Intravenous Sodium Bicarbonate and Oral N-acetylcysteine for the Prevention of Contrast-Induced Nephropathy
