Erythema Nodosum: Clinicopathologic Correlations and Their Use in Differential Diagnosis
- Affiliations
-
- 1Department of Dermatology, Ajou University School of Medicine, San 5 Wonchon- dong, Yeongtong-gu, Suwon 443-721, Korea. esl@ajou.ac.kr
- KMID: 2158164
- DOI: http://doi.org/10.3349/ymj.2007.48.4.601
Abstract
- PURPOSE
Typically, a diagnosis of erythema nodosum (EN) is based on clinical features. However, other diseases manifest with inflammatory nodules of the lower limbs in addition to EN, such as the EN-like lesions of Behcet's disease (BD). The purpose of this retrospective study was to investigate the frequency of histologically proven EN among diseases diagnosed clinically as EN, to determine underlying causes of EN, and to compare clinical and histologic features between EN and other diseases. PATIENTS AND METHODS: We selected 99 patients diagnosed clinically with EN and performed skin biopsies. All pathologic slides were evaluated and diagnosed; and after histologic diagnoses were made we reviewed the patients' medical records. RESULTS: Among the 99 patients diagnosed clinically with EN, 47 were biopsy-verified EN. The EN-like lesions of BD and nodular vasculitis were both in the primary differential diagnosis of EN. No definite difference in clinical features exists among these three diseases. Histologically, EN demonstrated septal panniculitis in the majority of patients. Lobular panniculitis was frequently observed in NV, and mixed or mostly lobular panniculitis was observed in the EN-like lesion. Vasculitis was rarely observed in EN; however lymphocytic vasculitis was observed frequently in EN-like lesions and neutrophilic vasculitis was observed in NV. The frequency of granulomatous inflammation was highest in NV. Some cases of patients with typical BD demonstrated classic EN lesions. CONSLUSION: It was extremely difficult to clinically differentiate EN from EN-like lesions or NV. We feel skin biopsy is mandatory for the diagnosis of lower extremity erythematous nodular lesions.
Keyword
MeSH Terms
Figure
-

Fig. 1 Clinical photographs of (A) EN, (B) EN-like lesion in BD, and (C) NV. Multiple, bilateral inflammatory subcutaneous nodules and plaques on the legs were observed. No ulceration was observed in these three diseases. No prominent differences were noted clinically.
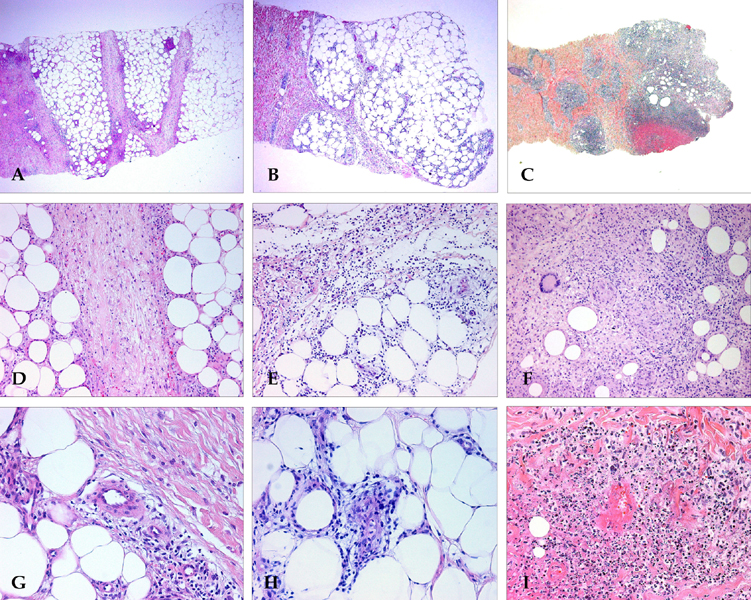
Fig. 2 Histopathologic findings of EN, EN-like lesion in BD, and NV. Pattern of panniculitis: Mostly septal panniculitis of EN (A, H & E stain, × 40). Inflammation presents mainly in and around the septa. Mixed septal and lobular panniculitis of EN-like lesion in BD (B, H & E stain, × 40). Inflammatory cells diffusely infiltrated in septa and lobules without clear compartmentalization. Mostly lobular panniculitis of NV (C, H & E stain, × 40). A region of caseation necrosis and surrounding inflammation replacing the septa and lobules was observed. Inflammation: There is an edema of the septa with paraseptal inflammation composed of lymphocytes mixed with histiocytes in EN (D, H & E stain, × 200). A dense inflammatory infiltrate of neutrophils mixed with lymphocytes was observed in the EN-like lesion (E, H & E stain, × 200). Severe lobular inflammation in NV (F, H & E stain, × 200), with extensive necrosis of adipocytes and granulomatous inflammation was observed. Vasculitis: No vasculitis was observed in EN (G, H & E stain, × 400). Lymphocytic vasculitis in EN-like lesion (H, H & E stain, × 400). Lymphocytic infiltrate around and within vessel wall was observed. Neutrophilic vasculitis in NV (I, H & E stain, × 400). Destruction of the vascular wall, surrounding neutrophils and nuclear dusts was observed.
Reference
-
1. Camilleri MJ, Su WPD. Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, editors. Panniculitis. Fitzpatrick's dermatology in general medicine. 2003. 6th ed. New York: McGraw-Hill;1047–1063.2. Tay YK. Erythema nodosum in Singapore. Clin Exp Dermatol. 2000. 25:377–380.
Article3. Barham KL, Jorizzo JL, Grattan B, Cox NH. Burns T, JBreathnach S, Cox N, Griffiths C, editors. Vasculitis and neutrophilic vascular reactions. Rook's textbook of dermatology. 2004. 7th ed. Oxford: Blackwell publishing;49.1–46.
Article4. Requena L, Yus ES. Panniculitis. Part I. Mostly septal panniculitis. J Am Acad Dermatol. 2001. 45:163–183. quiz 184–quiz 186.
Article5. Requena L, Sánchez Yus E. Panniculitis. Part II. Mostly lobular panniculitis. J Am Acad Dermatol. 2001. 45:325–361. quiz 362–quiz 364.
Article6. Bak H, Lee JW, Ahn HJ, Hwang SM, Choi EH, Lee SH, et al. An unusual case with membranous lipodystrophy in a hypertensive patient with transepidermal elimination. Yonsei Med J. 2006. 47:428–431.
Article7. Barnhill RL, Busam KJ, Nousari CH, Xu X, Barksdale SK. Elder DE, Elenitsas R, Johnson BL, Murphy GF, editors. Vascular diseases. Lever's histopathology of the skin. 2005. 9th ed. Philadelphia: Lippincott Williams & Wilkins;215–242.8. Carlson JA, Mihm MC, LeBoit PE. Cutaneous lympho-cytic vasculitis: a definition, a review, and a proposed classification. Semin Diagn Pathol. 1996. 13:72–90.9. International study group for Behçet's disease (ISGBD). Criteria for diagnosis of Behçet disease. Lancet. 1990. 335:1078–1080.10. Mert A, Ozaras R, Tabak F, Pekmezci S, Demirkesen C, Ozturk R. Erythema nodosum: an experience of 10 years. Scand J Infect Dis. 2004. 36:424–427.
Article11. Psychos DN, Voulgari PV, Skopouli FN, Drosos AA, Moutsopoulos HM. Erythema nodosum: the underlying conditions. Clin Rheumatol. 2000. 19:212–216.
Article12. García-Porrúa C, González-Gay MA, Vázquez-Caruncho M, López-Lazaro L, Luerio M, Fernández ML, et al. Erythema nodosum: etiologic and predictive factors in a defined population. Arthritis Rheum. 2000. 43:584–592.
Article13. Cribier B, Caille A, Heid E, Grosshans E. Erythema nodosum and associated diseases. A study of 129 cases. Int J Dermatol. 1998. 37:667–672.14. Tantisirin O, Puavilai S. Long-term follow-up of erythema nodosum. J Med Assoc Thai. 2003. 86:1095–1100.15. Global TB database. World Health Organization (WHO);Available from: http://www.who.int/tb/country/global_tb_database/en/index.html.16. Mizushima Y, Inaba G, Mimura Y, Ono S. Diagnostic criteria for Behçet's disease in 1987, and guideline for treating Behçet's disease. Saishin Igaku. 1988. 43:391–393.17. Kim YS, Kim SN. A clinical study on erythema nodosum and erythema induratum. Korean J Dermatol. 1984. 22:475–482.18. Choi US, Bang D, Lee KG, Chun SI. The clinical and histopathological study of erythema induratum and erythema nodosum. Korean J Dermatol. 1991. 29:304–312.19. Kim B, LeBoit PE. Histopathologic features of erythema nodosum-like lesions in Behçet's disease: a comparison with erythema nodosum focusing on the role of vasculitis. Am J Dermatopathol. 2000. 22:379–390.
Article20. Chun SI, Su WP, Lee S, Rogers RS. Erythema nodosum- like lesions in Behçet's syndrome: a histopathologic study of 30 cases. J Cutan Pathol. 1989. 16:259–265.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The clinical and histopatholgical study of erythema induratum and erythema nodosum
- Studies on the inflammatory Nodular Diseases of the Legs
- A Case of Erythema Nodosum Migrans
- Therapeutic Effect of Potassium Iodide in Erythema Nodosum
- Unusual Hypertrichosis Development on the Skin Involving Erythema Nodosum Migrans
