Trousseau's Syndrome in Association with Cholangiocarcinoma: Positive Tests for Coagulation Factors and Anticardiolipin Antibody
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, WHO Collaborating Center on Viral Hepatitis, The Catholic University of Korea, Seoul, Korea. yoonsk@catholic.ac.kr
- 2Department of Pathology, The Catholic University of Korea, Seoul, Korea.
- 3Department of Radiology, The Catholic University of Korea, Seoul, Korea.
- KMID: 2157800
- DOI: http://doi.org/10.3346/jkms.2006.21.1.155
Abstract
- Thromboembolic events are reported to occur with a high frequency in the setting of malignancy. However, reports on an association between cholangiocarcinoma and pulmonary thromboembolism, thus far, are almost lacking. We present here an unusual case of a 56-yr-old patient presenting cholangiocarcinoma and unexplained pulmonary thromboembolism. The patient had been quite healthy before the diagnosis. Coagulation tests showed elevated levels of fibrinogen, fibrinogen degradation product (FDP), D-dimer, and IgM anticardiolipin antibody (aCL Ab). The thromboemboli were resolved 3 weeks after anticoagulant therapy using lowmolecular-weight-heparin. Then, follow-up coagulation tests showed a marked decrease to normal in aCL Ab titer as well as the normalization of FDP and D-dimer levels. In this case, we describe pulmonary thromboembolism caused by hypercoagulable state associated with cholangiocarcinoma and speculate that such a thrombotic phenomenon could be regressed by anticoagulant therapy.
MeSH Terms
-
Antibodies, Anticardiolipin/blood
Anticoagulants/therapeutic use
Bile Duct Neoplasms/*complications
*Bile Ducts, Intrahepatic
Blood Coagulation Factors/analysis
Cholangiocarcinoma/*complications
Fibrin Fibrinogen Degradation Products/analysis
Fibrinogen/analysis
Heparin, Low-Molecular-Weight/therapeutic use
Humans
Male
Middle Aged
Pulmonary Embolism/*blood/drug therapy/etiology
Syndrome
Treatment Outcome
Figure
-
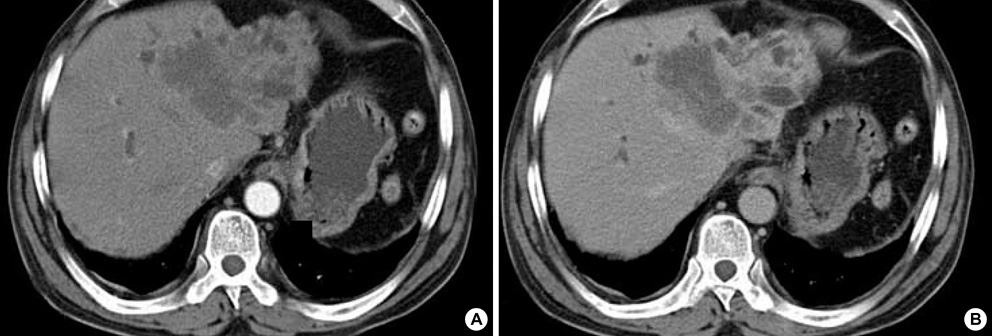
Fig. 1 Abdominal dynamic CT scan show about 6.5×7×7 cm-sized and ill-defined mass with several daughter nodules in the left lobe. The huge mass with a dilatation of intrahepatic bile ducts is not enhanced on the arterial phase (A), but shows delayed enhancement on the portal phase (B), indicating cholagiocarcinoma.

Fig. 2 Photomicrograph of liver biopsy specimens. Moderately differentiated adenocarcinoma is shown in the hematoxylin-eosin stain (A; original magnification ×100). On the immunohistochemical staining by using cytokeratin 19 (CK 19), dark-brown staining patterns are observed on the epithelium of proliferating bile ducts (B; original magnification ×400).

Fig. 3 Initial chest CT scan shows (A) a filling defect with lower density in the left interlobar pulmonary artery, indicating pulmonary thromboembolism. (B) Follow-up chest CT scan after anticoagulant therapy over 3 weeks revealed the interval regression of the thromboembolism.
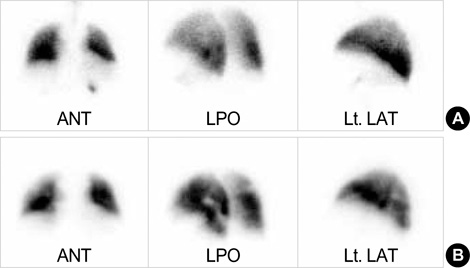
Fig. 4 Ventilation-perfusion scan reveals that no definite ventilatory abnormality in both lungs is shown (A), but multiple perfusion defects are found on the left lower lobe (B).
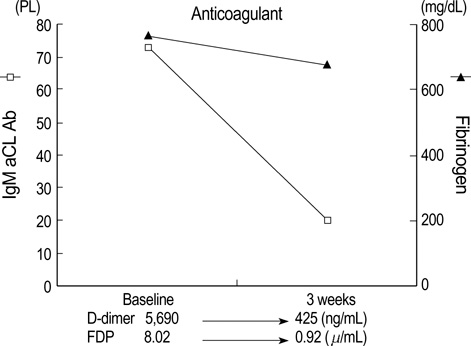
Fig. 5 Changes in FDP, D-dimer, fibrinogen, and aCL Ab levels during anticoagulant therapy. The levels of FDP, D-dimer, and aCL Ab were normalized, but fibrinogen level was slightly decreased.
Reference
-
1. Gores GJ. Cholangiocarcinoma: current concepts and insights. Hepatology. 2003. 37:961–969.
Article2. Hernandez JL, Riancho JA, Gonzalez-Macias J. Cholangiocarcinoma presenting as Trousseau's syndrome. Am J Gastroenterol. 1998. 93:847–848.3. Ching CK. Trousseau's syndrome in a patient with cholangiocarcinoma. Am J Gastroenterol. 1991. 86:928–929.4. Tasi SH, Juan CJ, Dai MS, Kao WY. Trousseau's syndrome related to adenocarcinoma of the colon and cholangiocarcinoma. Eur J Neurol. 2004. 11:493–496.
Article5. Sack GH Jr, Levin J, Bell WR. Trousseau's syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: clinical, pathophysiologic, and therapeutic features. Medicine (Baltimore). 1977. 56:1–37.6. Trousseau A. Phlegmasia Alba Dolens. Clinique medicale de l'Hotel-Dieu de Paris, London: New Syndeham Society. 1865. 3:94.7. Song MK, Kim YS, Lee KM, Kim SK, Chang J, Kim SK, Lee WY. A case of Trousseau's syndrome associated with lung cancer. Tuberc Respir Dis. 1995. 42:941–946.
Article8. Nakayama M, Iha T, Kanazawa K. Unusual Trousseau' syndrome in ovarian carcinosarcoma: multiple systemic thromboembolic events. J Obstet Gynaecol. 2002. 22:699–700.9. Walsh-McMonagle D, Green D. Low-molecular-weight heparin in the management of Trousseau's syndrome. Cancer. 1997. 80:649–655.10. Minna JD, Bunn PA Jr. DeVita VT, Hellman S, Rosenberg SA, editors. Paraneoplastic syndromes. Cancer: principles and practice of oncology. 1989. 3rd edition. Philadelphia: JB Lippincott;1920–1940.11. Denko NC, Giaccia AJ. Tumor hypoxia, the physiological link between Trousseau's syndrome (carcinoma-induced coagulopathy) and metastasis. Cancer Res. 2001. 61:795–798.12. Rogers LR, Cho ES, Kempin S, Posner JB. Cerebral infarction from non-bacterial thrombotic endocarditis. Clinical and pathological study including the effects of anticoagulation. Am J Med. 1987. 83:746–756.13. Levine JS, Branch DW, Rauch J. The antiphospholipid syndrome. N Engl J Med. 2002. 346:752–763.
Article14. von Tempelhoff GF, Heilmann L, Hommel G. Tumor hypoxia, the physiological link between Trousseau's syndrome (carcinoma-induced coagulopathy) and metastasis [letter]. Cancer Res. 2001. 61:7697–7698.15. Horan JT, Francis CW. Fibrin degradation products, fibrin monomer and soluble fibrin in disseminated intravascular coagulation. Semin Thromb Hemost. 2001. 27:657–666.
Article16. Kuruvilla J, Wells PS, Morrow B, MacKinnon K, Keeney M, Kovacs MJ. Prospective assessment of the natural history of positive D-dimer results in persons with acute venous thromboembolism (DVT or PE). Thromb Haemost. 2003. 89:284–287.
Article17. Runchey SS, Folsom AR, Tsai MY, Cushman M, McGovern PD. Anticardiolipin antibodies as a risk factor for venous thromboembolism in a population-based prospective study. Br J Haematol. 2002. 119:1005–1010.
Article18. Proven A, Bartlett RP, Moder KG, Chang-Miller A, Cardel LK, Heit JA, Homburger HA, Petterson TM, Christianson TJ, Nichols WL. Clinical importance of positive test results for lupus anticoagulant and anticardiolipin antibodies. Mayo Clin Proc. 2004. 79:467–475.
Article19. Caprini JA, Glase CJ, Anderson CB, Hathaway K. Laboratory markers in the diagnosis of venous thromboembolism. Circulation. 2004. 109:Suppl 1. I4–I8.
Article20. Zuckerman E, Toubi E, Golan TD, Rosenvald-Zuckerman T, Sabo E, Shmuel Z, Yeshurun D. Increased thromboembolic incidence in anti-cardiolipin-positive patients with malignancy. Br J Cancer. 1995. 72:447–451.
Article21. Morita S, Gebska MA, Kakkar AK, Scully MF. High affinity binding of heparin by necrotic tumour cells neutralises anticoagulant activity--implications for cancer related thromboembolism and heparin therapy. Thromb Haemost. 2001. 86:616–622.22. Zuger M, Demarmels Biasiutti F, Wuillemin WA, Furlan M, Lammle B. Subcutaneous low-molecular-weight heparin for treatment of Trousseau's syndrome. Ann Hematol. 1997. 75:165–167.
Article
