Endovascular Treatment for Type A Carotid Cavernous Fistulas with Detachable Coils
- Affiliations
-
- 1Department of Neurosurgery, Wonju College of Medicine, Yonsei University, Wonju, Korea. junghh@yonsei.ac.kr
- KMID: 2156154
- DOI: http://doi.org/10.13004/jknts.2008.4.2.77
Abstract
OBJECTIVE
Carotid cavernous fistulae (CCF) after head traumas are abnormal communications between the internal carotid artery and venous compartments of the cavernous sinus. Fistulae are uncommon but well-documented sequelae of craniofacial trauma. We report our experiences in placing detachable coils in the management of rare cases of direct CCF after head injuries.
METHODS
From January 2002 to December 2007, nine patients were admitted and treated for traumatic direct CCF at our hospital. The medical records and neuroimaging studies were retrospectively reviewed.
RESULTS
All 9 patients had previous head trauma histories and ocular symptoms including exophthalmos, conjunctiva injection, and chemosis. Angiography was performed to confirm the CCF and for treatment planning. According to the angiograph, three patients had pseudo-aneurysms. All of the patients were treated with detachable coils via the trans-arterial endovascular maneuver. Among them, two patients had recurrences, the first at postoperative day one and the other eleven days after the surgery. Both recurrences were retreated endovascularly. All nine patients were successfully treated anigographically by means of trans-arterial embolization and improved symptomatically within a week.
CONCLUSION
The etiology of CCF, especially type A, is well known. Also, the advances in interventional neuroradiology and cranial base surgery are chiefly responsible for the evolution of treatment strategies for CCF. Although other techniques and approaches with other materials may be useful, embolization with detachable coiling, as used in our cases, can be a safe and effective method to occlude the fistula and to improve symptoms.
MeSH Terms
Figure
-
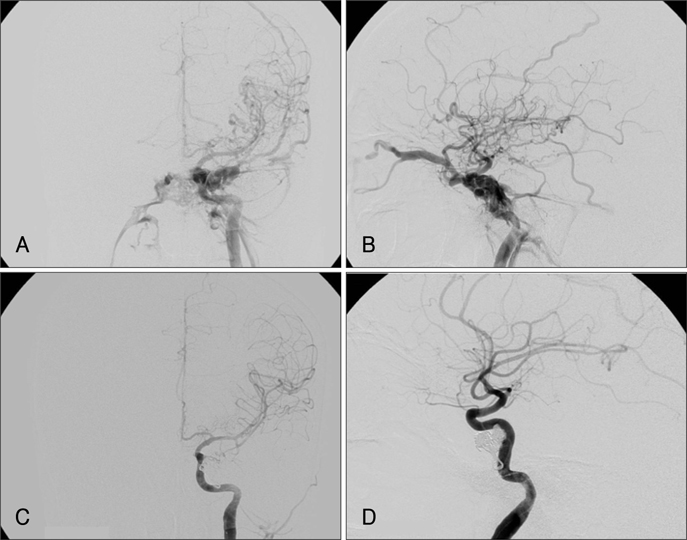
FIGURE 1 Pre- and post-operative arterial phase of the ICA angiogram in the case 2 patient. A and B: AP and lateral view of the pre-operative angiogram. Left ophthalmic vein, middle cerebral vein, inferior petrosal sinus, and pterygoid plexus are prominent in the arterial phase suggesting a high-flow CCF. C and D: AP and lateral view of the post-operative angiogram. Complete occlusion state of the CCF. CCF: carotid cavernous fistulae. ICA: internal carotid artery.
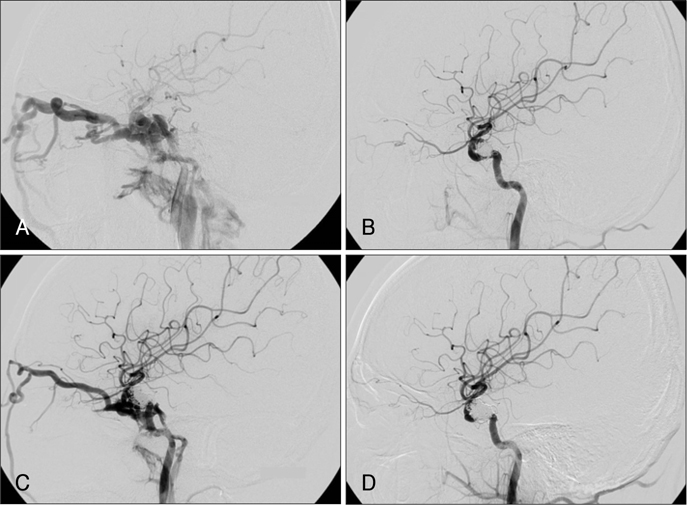
FIGURE 2 Pre- and post-operative arterial phase of the ICA angiogram in the case 6 patient. A: Pre-operative angiogram shows a prominent left ophthalmic vein, middle cerebral vein, inferior petrosal sinus, and pterygoid plexus. B: Post-operative angiogram shows complete occlusion of the CCF. C: Recurrence of the CCF is noted after the first embolization. D: Complete occlusion of the CCF after the 2nd procedure. CCF: carotid cavernous fistulae.
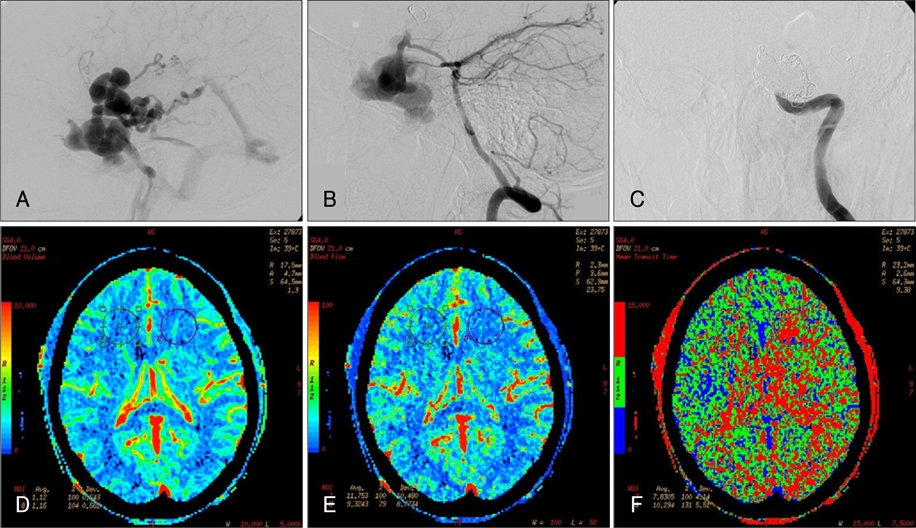
FIGURE 3 Pre- and post-operative arterial phase of the ICA angiogram and brain CT perfusion in the case 9 patient. A: Pseudoaneurysm and remarkable venous dilatation of the cavernous sinus including the petrosal sinus and pterygoid plexus is noted. B: Vertebral angiogram with manual compression of both the ICAs showing an aneurysm and fistulous drainage into the cavernous sinus. C: Complete occlusion of the ICA at the level of the aneurysm and complete obliteration of the aneurysm and CCF after the post-operative angiogram. D and F: Postembolization brain perfusion CT was revealed no perfusion defect in both hemisphere (D: Cerebral blood volume image, E: Cerebral blood flow image, F: Mean transit time image). ICA: internal carotid artery.
Reference
-
1. Abud DG, Spelle L, Piotin M, Mounayer C, Vanzin J, Moret J. Venous phase timing dura in balloon test occlusion as a criterion for permanent internal carotid artery sacrifice. AJNR Am J Neuroradiol. 2005; 26:2602–2609.2. Auyeung KM, Lui W, Chow L, Chan F. Massive epistaxis related to petrous carotid artery pseudoaneurysm after radiation therapy: emergency treatment with covered stent in two cases. AJNR Am J Neuroradiol. 2003; 24:1449–1452.3. Barrow DL, Spector R, Braun I, Tindall S, Tindall G. Classification and treatment of spontaneous carotid cavernous sinus fistulas. J Neurosurg. 1985; 62:248–256.4. Cheng KM, Chan C, Cheung Y, Chiu H, Tang K, Law C. Endovascular treatment of radiation-induced petrous internal carotid artery aneurysm presenting with acute haemorrhage: a report of two cases. Acta Neurochir (Wien). 2001; 143:351–355.
Article5. d'Angelo VA, Monte V, Scialfa G, Fiumara E, Scotti G. Intracerebral venous hemorrhage in "high-risk" carotid-cavernous fistula. Surg Neurol. 1988; 30:387–390.6. Day JD, Fukushima T. Direct microsurgery of dural arteriovenous malformation type carotid-cavernous sinus fistula: Indications, technique, and results. Neurosurgery. 1997; 41:1119–1124.7. Debrun GM. Treatment of traumatic carotid-cavernous fistula using detachable balloon catheters. AJNR Am J Neuroradiol. 1983; 4:355–356.8. Debrun GM, Vinuela F, Fox A, Davis K, Ahn H. Indications for treatment and classification of 132 carotid cavernous fistulas. Neurosurgery. 1988; 22:285–289.9. Fabian TS, Woody J, Ciraulo D, Lett E, Phlegar R, Barker D, et al. Posttraumatic carotid cavernous fistula: frequency analysis of signs, symptoms, and disability outcomes after angiographic embolization. J Trauma. 1999; 47:275–281.10. Forsting M, Sartor K. Hema and latex: a dangerous combination? Neuroradiology. 1991; 33:338–340.
Article11. Hara T, Hamada J, Kay Y, Ushio Y. Surgical transvenous embolization of a carotid-cavernous fistula with cortical drainage via a petrosal vein: two technical case reports. Neurosurgery. 2002; 50:1380–1383.12. Iida K, Uozumi T, Arita K, Nakahara T, Ohba S, Satoh H. Steal phenomenon in a traumatic carotid-cavernous fistula. J Trauma. 1995; 39:1015–1017.
Article13. Lewis AI, Tomsick T, Tew JJ. Management of 100 consecutive direct carotid-cavernous fistulas: results of treatment with detachable balloons. Neurosurgery. 1995; 36:239–244.14. Lewis AI, Tomsick T, Tew JM. Management of 100 consecutive direct carotid-cavernous fistulas: results of treatment with dieachable balloons. Neurosurgery. 1995; 36:239–245.15. Linskey ME, Jungreis C, Yonas H, Hirsch WJ, Sekhar L, Horton J, et al. Stroke risk after abrupt internal carotid artery sacrifice: accuracy of preoperative assessment with balloon test occlusion and stable xenon-enhanced CT. Am J Neuroradiol. 1994; 15:829–843.16. Manelfe C, Berenstein A. Treatment of carotid cavernous fistula by venous approach: report of two cases. J Neuroradiol. 1980; 7:13–19.17. Men S, Ozturk H, Hekimoglu B, Sekerci Z. Traumatic carotid cavernous fistula treated by combined transarterial and transvenous coil embolization and associated cavernous internal carotid artery dissection treated with stent placement. J Neurosurg. 2003; 99:584–586.18. Mericle RA, Lanzino G, Wakhioo A, Guterman L, Hopkins L. Stenting and secondary coiling of intracranial internal carotid artery aneurysm: technical case report. Neurosurgery. 1998; 43:1229–1234.
Article19. Miller NR, Monsieu L, Debrum G, Tamargo R, Nauta H. Treatment of carotid cavernous sinus fistula using a superior ophthalmic vein approach. J Neurosurg. 1995; 83:838–842.20. Miyachi S, Negoro M, Handa T, Terashima K, Keino H, Sugita K. Histopathological study of balloon embolization: silicone versus latex. Neurosurgery. 1992; 30:483–489.21. Monsein LH, Debrun G, Chazaly J. Hydroxyethyl methylacrylate and latex balloons. Am J Neuroradiol. 1990; 11:663–664.22. Morioka T, Matsushima T, Fujii K, Kukui M, Hasuo K, Hisashi K. Balloon test occlusion of the internal carotid artery with monitoring of compressed spectral arrays (CSAs) of electroencephalogram. Acta Neurochirurgica. 1989; 101:29–34.
Article23. Morris PP. Balloon reconstructive technique for the treatment of a carotid cavernous fistula. AJNR Am J Neuroradiol. 1999; 20:1107–1109.24. Mullan S. Treatment of carotid cavernous fistula by cavernous sinus occlusion. J Neurosurg. 1979; 50:131–144.25. Parkinson D. Carotid cavernous fistula: direct repair with preservation of the carotid artery-technical note. J Neurosurg. 1973; 38:99–106.26. Perez-Cruet MJ, Patwardhan R, Mawad M, Rose J. Treatment of dissecting pseudoaneurysm of the cervical internal carotid artery using a wall stent and detachable coils: case report. Neurosurgery. 1997; 40:622–626.
Article27. Phatouros CC, Sasaki T, Higashida R, Malek A, Meyers P, Dowd C, et al. Stent-supported coil embolization: the treatment of fusiform and wide-neck aneurysms and pseudoaneurysms. Neurosurgery. 2000; 47:107–115.
Article28. Redekop G, Marotta T, Weill A. Treatment of traumatic aneurysms and arteriovenous fistulas of the skull base by using endovascular stents. J Neurosurg. 2001; 95:412–419.
Article29. Sorteberg A, Sorteberg W, Bakke S, Lindegaard K, Boysen M, Nornes H. Cerebral haemodynamics in internal carotid artery trial occlusion. Acta Neurochirurgica. 1997; 139:1066–1073.
Article30. van Rooij WJ, Sluzewski M, Metz NH, Nijssen PC, Wijnalda D, Rinkel GJ, Tulleken CA. Carotid balloon occlusion for large and giant aneurysms: evaluation of a new test occlusion protocol. Neurosurgery. 2000; 47:116–121. discussion 122.
Article31. Viñuela F, Fox A, Debrum G, Peerless S, Drake C. Spontaneous carotid cavernous fistulas: clinical, radiological, and therapeutic considerations. Experience with 20 cases. J Neurosurg. 1984; 60:976–984.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Graft-Stent Placement for Treatment of Traumatic Carotid Cavernous Fistulas
- Direct Electrothrombosis of a Pseudoaneurysm after Obliteration of a Carotid Cavernous Fistula:Treatment with Guglielmi Detachable Coils: Case Report
- Transarterial Embolization of a Carotid Cavernous Fistula with Guglielmi Detachable Coils: A Case Report
- Endovascular Treatment of Direct Carotid Cavernous Fistulas Using Detachable Balloon(s) and Coils
- Superior ophthalmic approach in carotid-cavernous fistula: current concepts in indications, surgical techniques, and case reviews
