Cardiac Resynchronization Therapy and QRS Duration: Systematic Review, Meta-analysis, and Meta-regression
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine and Seoul National University Bundang Hospital, Seongnam, Korea.
- 2Department of Internal Medicine, Seoul National University College of Medicine and Seoul National University Hospital, Seoul, Korea. seil@snu.ac.kr
- 3Medical Research Collaborating Center, Seoul National University Hospital, Seoul, Korea.
- KMID: 2155444
- DOI: http://doi.org/10.3346/jkms.2015.30.1.24
Abstract
- Cardiac resynchronization therapy (CRT) has been shown to reduce the risk of death and hospitalization in patients with advanced heart failure with left ventricular dysfunction. However, controversy remains regarding who would most benefit from CRT. We performed a meta-analysis, and meta-regression in an attempt to identify factors that determine the outcome after CRT. A total of 23 trials comprising 10,103 patients were selected for this meta-analysis. Our analysis revealed that CRT significantly reduced the risk of all-cause mortality and hospitalization for heart failure compared to control treatment. The odds ratio (OR) of all-cause death had a linear relationship with mean QRS duration (P=0.009). The benefit in survival was confined to patients with a QRS duration > or =145 ms (OR, 0.86; 95% CI, 0.74-0.99), while no benefit was shown among patients with a QRS duration of 130 ms (OR, 1.00; 95% CI, 0.80-1.25) or less. Hospitalization for heart failure was shown to be significantly reduced in patients with a QRS duration > or =127 ms (OR, 0.77; 95% CI, 0.60-0.98). This meta-regression analysis implies that patients with a QRS duration > or =150 ms would most benefit from CRT, and in those with a QRS duration <130 ms CRT implantation may be potentially harmful.
MeSH Terms
-
Bundle-Branch Block/physiopathology
Cardiac Resynchronization Therapy/*methods
Cardiac Resynchronization Therapy Devices
Defibrillators, Implantable
Electrocardiography
Heart Failure/mortality/physiopathology/*therapy
Humans
Myocardial Contraction/*physiology
Treatment Outcome
Ventricular Dysfunction, Left/mortality/physiopathology/*therapy
Figure
-

Fig. 1 Flow diagram of systematic review. The flow diagram depicts the detailed process of systematic literature review according the statement of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. RCT, randomized controlled trial.
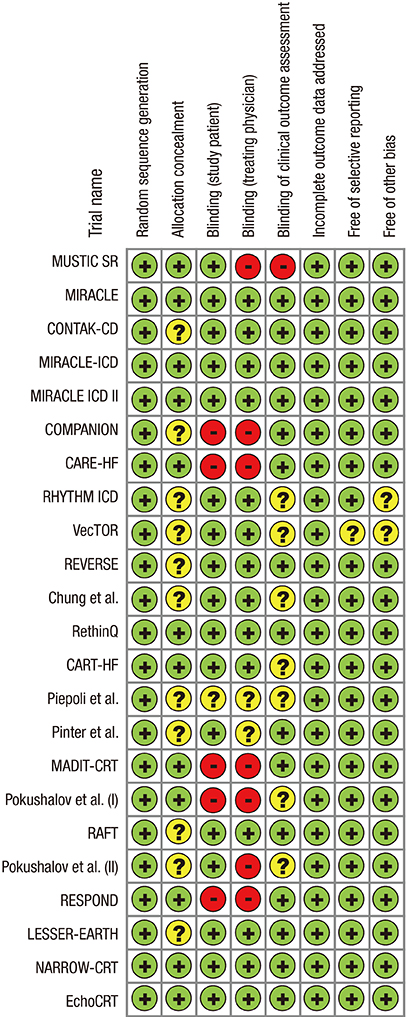
Fig. 2 Risk of bias assessment. Risk of bias of each included trial was assessed with the Cochrane Collaboration's tool. This 'risk of bias' summary presents all of the judgments in a cross-tabulation of study by entry. Green represents 'Yes (low risk of bias)'; yellow, 'Unclear'; red, 'No (high risk of bias)'.

Fig. 3 Meta-analysis and meta-regression for all-cause mortality. (A) Forest plot with odds ratios (OR) for all-cause death after cardiac resynchronization therapy (CRT) compared to control treatment for individual trials and the pooled population. The squares and the horizontal lines indicate the ORs and the 95% confidence intervals (CI) for each included trial. The size of each square is proportional to the statistical weight of a trial in the meta-analysis. A diamond indicates the effect estimate derived from the meta-analysis, with the center indicating the point estimate and the left and the right ends the 95% CI. (B) OR of CRT compared to control as a function of the mean QRS duration of participants at enrollment. ORs are displayed on a logarithmic scale. Circles represent the individual studies, and the size of each circle is proportional to the statistical weight of a trial in the meta-analysis. The fitted meta-regression function is drawn in a solid line accompanied by the upper and lower bounds for the 95% mean prediction interval (dotted lines).
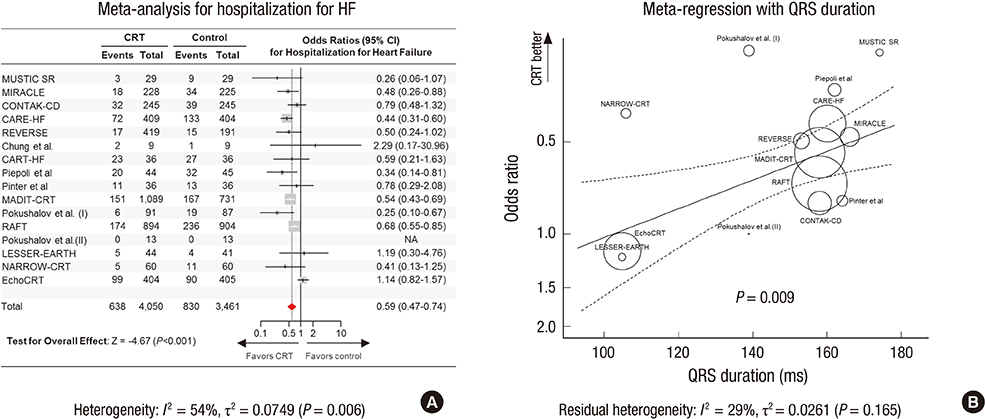
Fig. 4 Meta-analysis and meta-regression for hospitalization for heart failure (HF). (A) Forest plot with odds ratios (OR) for hospitalization for HF after cardiac resynchronization therapy (CRT) compared to control treatment for individual trials and the pooled population. The squares and the horizontal lines indicate the ORs and the 95% confidence intervals (CI) for each trial included. The size of each square is proportional to the statistical weight of a trial in the meta-analysis. A diamond indicates the effect estimate derived from the meta-analysis, with the center indicating the point estimate and the left and the right ends the 95% CI. (B) OR for HF hospitalization after CRT compared to control as a function of the mean QRS duration of participants at enrollment. ORs are displayed on a logarithmic scale. Circles represent the individual studies, and the size of each circle is proportional to the statistical weight of the trial in the meta-analysis. The fitted meta-regression function is drawn in a solid line accompanied by the upper and lower bounds for the 95% mean prediction interval (dotted lines).
Cited by 1 articles
-
The Past, Present and Future of Cardiac Resynchronization Therapy
Thomas O'Brien, Myung-Soo Park, Jong-Chan Youn, Eugene S. Chung
Korean Circ J. 2019;49(5):384-399. doi: 10.4070/kcj.2019.0114.
Reference
-
1. Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statisticsz: 2012 update: a report from the American Heart Association. Circulation. 2012; 125:e2–e220.2. Cazeau S, Ritter P, Bakdach S, Lazarus A, Limousin M, Henao L, Mundler O, Daubert JC, Mugica J. Four chamber pacing in dilated cardiomyopathy. Pacing Clin Electrophysiol. 1994; 17:1974–1979.3. Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, Mancini DM. Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation. Circulation. 1997; 95:2660–2667.4. Linde C, Abraham WT, Gold MR, John John M St, Ghio S, Daubert C. REVERSE (REsynchronization reVErses Remodeling in Systolic left vEntricular dysfunction) Study Group. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008; 52:1834–1843.5. Cazeau S, Leclercq C, Lavergne T, Walker S, Varma C, Linde C, Garrigue S, Kappenberger L, Haywood GA, Santini M, et al. Multisite Stimulation in Cardiomyopathies (MUSTIC) Study Investigators. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med. 2001; 344:873–880.6. Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, Kocovic DZ, Packer M, Clavell AL, Hayes DL, et al. MIRACLE Study Group. Multicenter InSync Randomized Clinical Evaluation. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002; 346:1845–1853.7. Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, Carson P, DiCarlo L, DeMets D, White BG, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004; 350:2140–2150.8. Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappenberger L, Tavazzi L. Cardiac Resynchronization-Heart Failure (CARE-HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005; 352:1539–1549.9. Tracy CM, Epstein AE, Darbar D, DiMarco JP, Dunbar SB, Estes NA 3rd, Ferguson TB Jr, Hammill SC, Karasik PE, Link MS, et al. American College of Cardiology Foundation. American Heart Association Task Force on Practice Guidelines. Heart Rhythm Society. 2012 ACCF/AHA/HRS focused update of the 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. [corrected]. Circulation. 2012; 126:1784–1800.10. Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, Cleland J, Deharo JC, Delgado V, Elliott PM, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013; 34:2281–2329.11. Sipahi I, Carrigan TP, Rowland DY, Stambler BS, Fang JC. Impact of QRS duration on clinical event reduction with cardiac resynchronization therapy: meta-analysis of randomized controlled trials. Arch Intern Med. 2011; 171:1454–1462.12. Gervais R, Leclercq C, Shankar A, Jacobs S, Eiskjaer H, Johannessen A, Freemantle N, Cleland JG, Tavazzi L, Daubert C. CARE-HF investigators. Surface electrocardiogram to predict outcome in candidates for cardiac resynchronization therapy: a sub-analysis of the CARE-HF trial. Eur J Heart Fail. 2009; 11:699–705.13. Zareba W, Klein H, Cygankiewicz I, Hall WJ, McNitt S, Brown M, Cannom D, Daubert JP, Eldar M, Gold MR, et al. MADIT-CRT Investigators. Effectiveness of Cardiac Resynchronization Therapy by QRS Morphology in the Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy (MADIT-CRT). Circulation. 2011; 123:1061–1072.14. Beshai JF, Grimm RA, Nagueh SF, Baker JH 2nd, Beau SL, Greenberg SM, Pires LA, Tchou PJ. Cardiac-resynchronization therapy in heart failure with narrow QRS complexes. N Engl J Med. 2007; 357:2461–2471.15. Foley PW, Patel K, Irwin N, Sanderson JE, Frenneaux MP, Smith RE, Stegemann B, Leyva F. Cardiac resynchronisation therapy in patients with heart failure and a normal QRS duration: the RESPOND study. Heart. 2011; 97:1041–1047.16. Thibault B, Harel F, Ducharme A, White M, Ellenbogen KA, Frasure-Smith N, Roy D, Philippon F, Dorian P, Talajic M, et al. LESSER-EARTH Investigators. Cardiac resynchronization therapy in patients with heart failure and a QRS complex <120 milliseconds: the Evaluation of Resynchronization Therapy for Heart Failure (LESSER-EARTH) trial. Circulation. 2013; 127:873–881.17. Muto C, Solimene F, Gallo P, Nastasi M, La Rosa C, Calvanese R, Iengo R, Canciello M, Sangiuolo R, Diemberger I, et al. A randomized study of cardiac resynchronization therapy defibrillator versus dual-chamber implantable cardioverter-defibrillator in ischemic cardiomyopathy with narrow QRS: the NARROW-CRT study. Circ Arrhythm Electrophysiol. 2013; 6:538–545.18. Ruschitzka F, Abraham WT, Singh JP, Bax JJ, Borer JS, Brugada J, Dickstein K, Ford I, Gorcsan J 3rd, Gras D, et al. EchoCRT Study Group. Cardiac-resynchronization therapy in heart failure with a narrow QRS complex. N Engl J Med. 2013; 369:1395–1405.19. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. the Cochrane Collaboration;updated March 2011. accessed on 06 December 2013. Available at http://www.cochrane-handbook.org/.20. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986; 7:177–188.21. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003; 327:557–560.22. Thompson SG, Sharp SJ. Explaining heterogeneity in meta-analysis: a comparison of methods. Stat Med. 1999; 18:2693–2708.23. NICE Decision Support Unit. Heterogeneity: subgroups, meta-regression, bias and bias-adjustment. accessed on 06 December 2013. Available at http://www.nicedsu.org.uk/TSD3%20Heterogeneity.final%20report.08.05.12.pdf.24. Jonas DE, Wilkins TM, Bangdiwala S, Bann CM, Morgan LC, Thaler KJ, Amick HR, Gartlehner G. Findings of Bayesian mixed treatment comparison meta-analyses: comparison and exploration using real-world trial data and simulation. accessed on 06 December 2013. Available at http://www.ncbi.nlm.nih.gov/books/NBK126104/.25. Gelman A, Rubin DB. Inference from iterative simulation using multiple sequences. Stat Sci. 1992; 457–472.26. Pokushalov E, Romanov A, Prohorova D, Cherniavsky A, Goscinska-Bis K, Bis J, Bochenek A, Karaskov A. Coronary artery bypass grafting with concomitant cardiac resynchronisation therapy in patients with ischaemic heart failure and left ventricular dyssynchrony. Eur J Cardiothorac Surg. 2010; 38:773–780.27. Pokushalov E, Romanov A, Corbucci G, Prohorova D, Chernyavsky A, Larionov P, Terekhov I, Artyomenko S, Kliver E, Shirokova N, et al. Cardiac resynchronization therapy and bone marrow cell transplantation in patients with ischemic heart failure and electromechanical dyssynchrony: a randomized pilot study. J Cardiovasc Transl Res. 2011; 4:767–778.28. Summary of Safety and Effectiveness Data: St. Jude Epic and Atlas+HF CRT-D Systems. accessed on 02 November 2013. Available at http://www.fda.gov/ohrms/dockets/dockets/05m0492/05m-0492-aav0001-03-SSED-vol1.pdf.29. Summary of Safety and Effectiveness Data: St. Jude Frontier Cardiac Resynchronizatio Therapy. accessed on 02 November 2013. Available at http://www.fda.gov/ohrms/dockets/dockets/05m0289/05m-0289-aav0001-03-SSED-vol1.pdf.30. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE Jr, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013; 128:1810–1852.31. Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, Estes NA 3rd, Foster E, Greenberg H, Higgins SL, et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009; 361:1329–1338.32. Tang AS, Wells GA, Talajic M, Arnold MO, Sheldon R, Connolly S, Hohnloser SH, Nichol G, Birnie DH, Sapp JL, et al. Resynchronization-Defibrillation for Ambulatory Heart Failure Trial Investigators. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med. 2010; 363:2385–2395.33. Yu CM, Lin H, Zhang Q, Sanderson JE. High prevalence of left ventricular systolic and diastolic asynchrony in patients with congestive heart failure and normal QRS duration. Heart. 2003; 89:54–60.34. Ku SY, Cho GY, Han SW, Choi SH, Park WJ, Doo YC, Hong KS, Oh DJ, Lee Y. Doppler tissue image for diagnosis of myocardial dyssynchronicity in congestive heart failure: comparison with EKG. Korean Circ J. 2004; 34:388–394.35. McAlister FA, Ezekowitz J, Hooton N, Vandermeer B, Spooner C, Dryden DM, Page RL, Hlatky MA, Rowe BH. Cardiac resynchronization therapy for patients with left ventricular systolic dysfunction: a systematic review. JAMA. 2007; 297:2502–2514.36. Al-Majed NS, McAlister FA, Bakal JA, Ezekowitz JA. Meta-analysis: cardiac resynchronization therapy for patients with less symptomatic heart failure. Ann Intern Med. 2011; 154:401–412.37. Yancy CW, McMurray JJ. ECG: still the best for selecting patients for CRT. N Engl J Med. 2013; 369:1463–1464.38. Thompson SG, Higgins JP. How should meta-regression analyses be undertaken and interpreted? Stat Med. 2002; 21:1559–1573.39. Gold MR, Thébault C, Linde C, Abraham WT, Gerritse B, Ghio S, John Sutton M St, Daubert JC. Effect of QRS duration and morphology on cardiac resynchronization therapy outcomes in mild heart failure: results from the Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction (REVERSE) study. Circulation. 2012; 126:822–829.40. Sipahi I, Chou JC, Hyden M, Rowland DY, Simon DI, Fang JC. Effect of QRS morphology on clinical event reduction with cardiac resynchronization therapy: meta-analysis of randomized controlled trials. Am Heart J. 2012; 163:260–267.e3.41. Singh JP, Klein HU, Huang DT, Reek S, Kuniss M, Quesada A, Barsheshet A, Cannom D, Goldenberg I, McNitt S, et al. Left ventricular lead position and clinical outcome in the multicenter automatic defibrillator implantation trial-cardiac resynchronization therapy (MADIT-CRT) trial. Circulation. 2011; 123:1159–1166.42. Higgins SL, Hummel JD, Niazi IK, Giudici MC, Worley SJ, Saxon LA, Boehmer JP, Higginbotham MB, De Marco T, Foster E, et al. Cardiac resynchronization therapy for the treatment of heart failure in patients with intraventricular conduction delay and malignant ventricular tachyarrhythmias. J Am Coll Cardiol. 2003; 42:1454–1459.43. Young JB, Abraham WT, Smith AL, Leon AR, Lieberman R, Wilkoff B, Canby RC, Schroeder JS, Liem LB, Hall S, et al. Multicenter InSync ICD Randomized Clinical Evaluation (MIRACLE ICD) Trial Investigators. Combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA. 2003; 289:2685–2694.44. Abraham WT, Young JB, León AR, Adler S, Bank AJ, Hall SA, Lieberman R, Liem LB, O'Connell JB, Schroeder JS, et al. Multicenter InSync ICD II Study Group. Effects of cardiac resynchronization on disease progression in patients with left ventricular systolic dysfunction, an indication for an implantable cardioverter-defibrillator, and mildly symptomatic chronic heart failure. Circulation. 2004; 110:2864–2868.45. Chung ES, Menon SG, Weiss R, Schloss EJ, Chow T, Kereiakes DJ, Mazur W, Salo RW, Galle E, Pastore JM. Feasibility of biventricular pacing in patients with recent myocardial infarction: impact on ventricular remodeling. Congest Heart Fail. 2007; 13:9–15.46. Bentkover JD, Dorian P, Thibault B, Gardner M. Economic analysis of a randomized trial of biventricular pacing in Canada. Pacing Clin Electrophysiol. 2007; 30:38–43.47. Piepoli MF, Villani GQ, Corrà U, Aschieri D, Rusticali G. Time course of effects of cardiac resynchronization therapy in chronic heart failure: benefits in patients with preserved exercise capacity. Pacing Clin Electrophysiol. 2008; 31:701–708.48. Pinter A, Mangat I, Korley V, Connolly S, Connors S, Gardner M, Philippon F, Sterns L, Thibault B, Dorian P. Assessment of resynchronization therapy on functional status and quality of life in patients requiring an implantable defibrillator. Pacing Clin Electrophysiol. 2009; 32:1509–1519.
