Korean J Urol.
2015 May;56(5):398-404. 10.4111/kju.2015.56.5.398.
Is a secondary procedure necessary in every case of failed endoscopic treatment for vesicoureteral reflux?
- Affiliations
-
- 1Department of Urology, Catholic University of Daegu School of Medicine, Daegu, Korea.
- 2Department of Urology and Urological Science Institute, Yonsei University College of Medicine, Seoul, Korea. swhan@yuhs.ac
- 3Department of Urology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2155321
- DOI: http://doi.org/10.4111/kju.2015.56.5.398
Abstract
- PURPOSE
Endoscopic treatment (ET) has become a widely accepted procedure for treating vesicoureteral reflux (VUR). However, patients followed up after ET over long periods have reported persistent or recurrent VUR. We evaluated the natural course of failed ET in patients who required further treatments to help physicians in making decisions on the treatment of VUR.
MATERIALS AND METHODS
We retrospectively reviewed the medical records of patients who were diagnosed with VUR and underwent ET from January 2006 to December 2009. A total of 165 patients with 260 ureters underwent ET. We compared the parameters of the patients according to ET success or failure and evaluated the natural course of the patients after ET failure.
RESULTS
Mean VUR grade and positive photon defect were higher in the failed ET group than in the successful ET group. Six months after the operation, persistent or recurrent VUR was observed in 76 ureters (29.2%), and by 16.3 months after the operation, VUR resolution was observed in 18 ureters (23.7%). Twenty-five ureters (32.9%) without complications were observed conservatively. Involuntary detrusor contraction was found in 1 of 9 (11.1%) among the secondary ET success group, whereas in the secondary ET failure group, 4 of 6 (66.7%) had accompanying involuntary detrusor contraction.
CONCLUSIONS
Patients in whom ET fails can be observed for spontaneous resolution of VUR unless they have febrile urinary tract infection or decreased renal function. Urodynamic study may be helpful in deciding whether a secondary procedure after ET failure is necessary.
Keyword
MeSH Terms
Figure
-
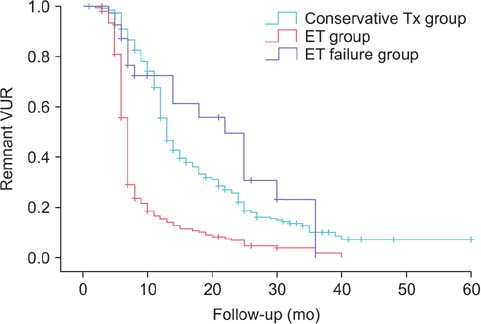
Fig. 1 Vesicoureteral reflux (VUR) resolution curve. VUR resolution occurred in 21.01±2.36 months after endoscopic treatment (ET), which was not significantly different from 18.8±0.97 months for the conservative treatment group (p=0.42). Number of patients in each group: conservative treatment (Tx) group (n=309), ET group (n=260), and ET failure group (n=76).

Fig. 2 Algorithm of treatment for failed endoscopic treatment (ET). A secondary procedure was performed in cases of recurrent febrile urinary tract infection or newly developed renal scarring or a decrease in renal function after ET failure. When a newly developed renal scar or decreased renal function was observed, we performed ureteral reimplantation rather than secondary ET.
Reference
-
1. Lackgren G, Wahlin N, Skoldenberg E, Stenberg A. Long-term followup of children treated with dextranomer/hyaluronic acid copolymer for vesicoureteral reflux. J Urol. 2001; 166:1887–1892.2. Elder JS, Shah MB, Batiste LR, Eaddy M. Part 3: Endoscopic injection versus antibiotic prophylaxis in the reduction of urinary tract infections in patients with vesicoureteral reflux. Curr Med Res Opin. 2007; 23:Suppl 4. S15–S20.3. Molitierno JA, Scherz HC, Kirsch AJ. Endoscopic treatment of vesicoureteral reflux using dextranomer hyaluronic acid copolymer. J Pediatr Urol. 2008; 4:221–228.4. Lee EK, Gatti JM, Demarco RT, Murphy JP. Long-term follow-up of dextranomer/hyaluronic acid injection for vesicoureteral reflux: late failure warrants continued followup. J Urol. 2009; 181:1869–1874.5. Higham-Kessler J, Reinert SE, Snodgrass WT, Hensle TW, Koyle MA, Hurwitz RS, et al. A review of failures of endoscopic treatment of vesicoureteral reflux with dextranomer microspheres. J Urol. 2007; 177:710–714.6. Sedberry-Ross S, Rice DC, Pohl HG, Belman AB, Majd M, Rushton HG. Febrile urinary tract infections in children with an early negative voiding cystourethrogram after treatment of vesicoureteral reflux with dextranomer/hyaluronic acid. J Urol. 2008; 180:4 Suppl. 1605–1609.7. Mendez R, Somoza I, Tellado MG, Liras J, Sanchez A, Pais E, et al. Predictive value of clinical factors for successful endoscopic correction of primary vesicoureteral reflux grades III-IV. J Pediatr Urol. 2006; 2:545–550.8. Alkan M, Ciftci AO, Senocak ME, Tanyel FC, Buyukpamukcu N. Endoscopic treatment of vesicoureteral reflux in children: our experience and analysis of factors affecting success rate. Urol Int. 2008; 81:41–46.9. Lee DW, Kang KM, Oh WS, Kim JS, Chung SK. Risk factors for treatment failure after endoscopic subureteral injection of dextranomer/hyaluronic acid copolymer (Deflux(R)) for vesicoureteral reflux. Korean J Urol. 2009; 50:61–66.10. Taylor CM, Corkery JJ, White RH. Micturition symptoms and unstable bladder activity in girls with primary vesicoureteric reflux. Br J Urol. 1982; 54:494–498.11. Koff SA, Murtagh DS. The uninhibited bladder in children: effect of treatment on recurrence of urinary infection and on vesicoureteral reflux resolution. J Urol. 1983; 130:1138–1141.12. Yeung CK, Sreedhar B, Sihoe JD, Sit FK. Renal and bladder functional status at diagnosis as predictive factors for the outcome of primary vesicoureteral reflux in children. J Urol. 2006; 176:1152–1156.13. Kraft KH, Molitierno JA Jr, Dewhurst L, Geers C, Gunderson K, Scherz HC, et al. Is endoscopic injection therapy a reasonable treatment option for low-grade vesicoureteral reflux in association with overactive bladder? Urology. 2011; 78:675–678.14. Medical versus surgical treatment of primary vesicoureteral reflux: report of the International Reflux Study Committee. Pediatrics. 1981; 67:392–400.15. Koff SA. Estimating bladder capacity in children. Urology. 1983; 21:248.16. Neveus T, von Gontard A, Hoebeke P, Hjalmas K, Bauer S, Bower W, et al. The standardization of terminology of lower urinary tract function in children and adolescents: report from the Standardisation Committee of the International Children's Continence Society. J Urol. 2006; 176:314–324.17. Matouschek E. New concept for the treatment of vesico-ureteral reflux. Endoscopic application of teflon. Arch Esp Urol. 1981; 34:385–388.18. O'Donnell B, Puri P. Treatment of vesicoureteric reflux by endoscopic injection of Teflon. 1984. J Urol. 2002; 167:1808–1809.19. Stenberg A, Lackgren G. A new bioimplant for the endoscopic treatment of vesicoureteral reflux: experimental and short-term clinical results. J Urol. 1995; 154(2 Pt 2):800–803.20. Kirsch AJ, Perez-Brayfield M, Smith EA, Scherz HC. The modified sting procedure to correct vesicoureteral reflux: improved results with submucosal implantation within the intramural ureter. J Urol. 2004; 171(6 Pt 1):2413–2416.21. Lavelle MT, Conlin MJ, Skoog SJ. Subureteral injection of Deflux for correction of reflux: analysis of factors predicting success. Urology. 2005; 65:564–567.22. Yucel S, Gupta A, Snodgrass W. Multivariate analysis of factors predicting success with dextranomer/hyaluronic acid injection for vesicoureteral reflux. J Urol. 2007; 177:1505–1509.23. Kajbafzadeh AM, Tourchi A, Aryan Z. Factors that impact the outcome of endoscopic correction of vesicoureteral reflux: a multivariate analysis. Int Urol Nephrol. 2013; 45:1–9.24. Puri P, Chertin B, Velayudham M, Dass L, Colhoun E. Treatment of vesicoureteral reflux by endoscopic injection of dextranomer/hyaluronic Acid copolymer: preliminary results. J Urol. 2003; 170(4 Pt 2):1541–1544.25. Chi A, Gupta A, Snodgrass W. Urinary tract infection following successful dextranomer/hyaluronic acid injection for vesicoureteral reflux. J Urol. 2008; 179:1966–1969.26. Capozza N, Lais A, Matarazzo E, Nappo S, Patricolo M, Caione P. Influence of voiding dysfunction on the outcome of endoscopic treatment for vesicoureteral reflux. J Urol. 2002; 168(4 Pt 2):1695–1698.27. Bachelard M, Sillen U, Hansson S, Hermansson G, Jodal U, Jacobsson B. Urodynamic pattern in asymptomatic infants: siblings of children with vesicoureteral reflux. J Urol. 1999; 162:1733–1737.28. Jansson UB, Hanson M, Hanson E, Hellström AL, Sillen U. Voiding pattern in healthy children 0 to 3 years old: a longitudinal study. J Urol. 2000; 164:2050–2054.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endoscopic teflon injection in vesicoureteral reflux
- Secondary surgery for vesicoureteral reflux after failed endoscopic injection: Comparison to primary surgery
- Clinical Observation on Vesicoureteral Reflex Following Renal Tuberculosis
- Clinical Aspects of Vesicoureteral Reflux
- Transient Pseudohypoaldosteronism in an Infant with Vesicoureteral Reflux
