Treatment of Unstable Osteochondral Dissecans Lesion of the Knee Joint Using Autologous Osteochondral Plug
- Affiliations
-
- 1Department of Orthopedic Surgery, Bumin General Hospital, Busan, Korea. kdh7483@gmail.com
- 2Department of Orthopedic Surgery, Veterans Hospital, Busan, Korea.
- KMID: 2154351
- DOI: http://doi.org/10.4055/jkoa.2016.51.1.69
Abstract
- PURPOSE
The purpose of this study was to evaluate the clinical results of fixation of the unstable osteochondral dissecans (OCD) lesion with autologous osteochondral plugs.
MATERIALS AND METHODS
This study was conducted in 19 patients who were relevant to the International Cartilage Repair Society 2, 3, or 4 who were treated with autologous osteochondral plugs and followed-up for more than 2 years from January 2004 to January 2012. Clinical evaluation was performed by comparing the preoperative and last follow-up scores of Lysholm score and subjective International Knee Documentation Committee (IKDC) score.
RESULTS
All patients were male and the average age was 19.1 years. Of the 19 cases, there were 16 cases of medial femoral condyle lateral side lesion, 2 cases of lateral femoral condyle articular surface, and 1 case of femoral intercondylar notch lesions. The average size of the lesion was 5.68 mm2, and average use of osteochodral plugs were 4.3. Average follow-up period was 38 months. Preoperative Lysholm score, IKDC subjective score showed significant improvement.
CONCLUSION
Fixation with autologous osteochondral plugs for unstable OCD uses the remnant tissues therefore conserving it, which is thought to be the positive aspect of this type of operation.
Figure
-
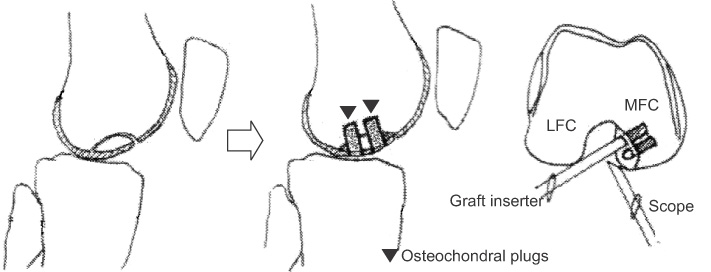
Figure 1 Mosaicplasty was performed and a osteochondral plug with 4.5 mm in diameter was collected and fixed at the center of the cartilage. To maintain stability an additional 4.5 mm or depending on the remnant surface, 3.5 mm or 2.7 mm osteochondral plug was fixed at the margins. LFC, lateral femoral condyle; MFC, medial femoral condyle.
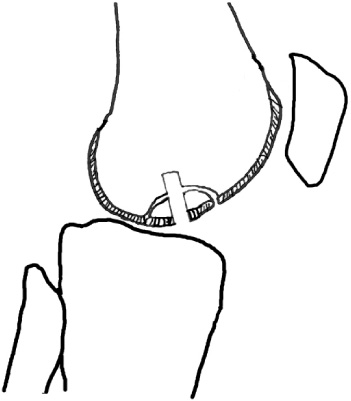
Figure 2 A 4.5 mm drill was used to drill the subchondral bone sufficient enough for fixation.
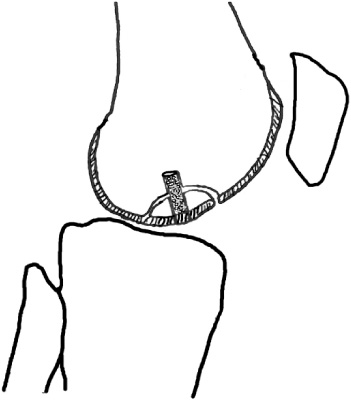
Figure 3 A guide tube was used to insert the osteochondral plug to match the cartilage portion of the plug and the lesion.
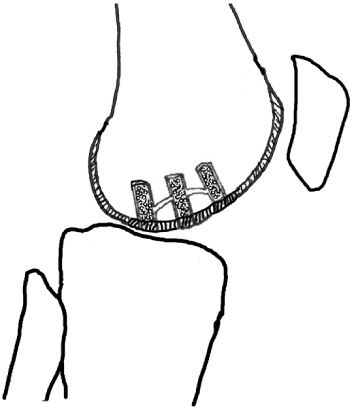
Figure 4 The outer margin was firmly fixed with osteochondral plugs using the same method.
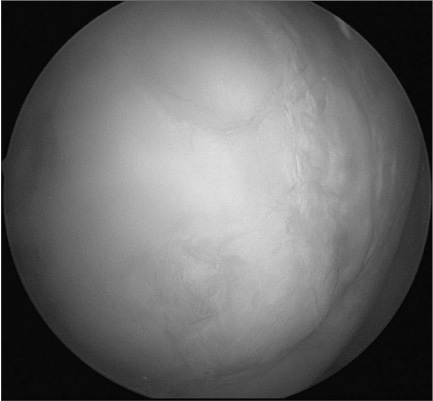
Figure 5 Complete healing state on 2nd look arthroscopic finding at 12 months follow-up.
Reference
-
1. Williams JS Jr, Bush-Joseph CA, Bach BR Jr. Osteochondritis dissecans of the knee. Am J Knee Surg. 1998; 11:221–232.2. Berlet GC, Mascia A, Miniaci A. Treatment of unstable osteochondritis dissecans lesions of the knee using autogenous osteochondral grafts (mosaicplasty). Arthroscopy. 1999; 15:312–316.
Article3. Clanton TO, DeLee JC. Osteochondritis dissecans History, pathophysiology and current treatment concepts. Clin Orthop Relat Res. 1982; 167:50–64.
Article4. Lindén B. The incidence of osteochondritis dissecans in the condyles of the femur. Acta Orthop Scand. 1976; 47:664–667.
Article5. Schenck RC Jr, Goodnight JM. Osteochondritis dissecans. J Bone Joint Surg Am. 1996; 78:439–456.6. Yamashita F, Sakakida K, Suzu F, Takai S. The transplantation of an autogeneic osteochondral fragment for osteochondritis dissecans of the knee. Clin Orthop Relat Res. 1985; 201:43–50.
Article7. Hughston JC, Hergenroeder PT, Courtenay BG. Osteochondritis dissecans of the femoral condyles. J Bone Joint Surg Am. 1984; 66:1340–1348.
Article8. Linden B. Osteochondritis dissecans of the femoral condyles: a long-term follow-up study. J Bone Joint Surg Am. 1977; 59:769–776.9. Aglietti P, Ciardullo A, Giron F, Ponteggia F. Results of arthroscopic excision of the fragment in the treatment of osteochondritis dissecans of the knee. Arthroscopy. 2001; 17:741–746.
Article10. Anderson AF, Richards DB, Pagnani MJ, Hovis WD. Antegrade drilling for osteochondritis dissecans of the knee. Arthroscopy. 1997; 13:319–324.
Article11. Miura K, Ishibashi Y, Tsuda E, Sato H, Toh S. Results of arthroscopic fixation of osteochondritis dissecans lesion of the knee with cylindrical autogenous osteochondral plugs. Am J Sports Med. 2007; 35:216–222.
Article12. Hefti F, Müller W. Current state of evaluation of knee ligament lesions. The new IKDC knee evaluation form. Orthopade. 1993; 22:351–362.13. Anderson AF, Lipscomb AB, Coulam C. Antegrade curettement, bone grafting and pinning of osteochondritis dissecans in the skeletally mature knee. Am J Sports Med. 1990; 18:254–261.
Article14. Green WT, Banks HH. Osteochondritis dissecans in children. J Bone Joint Surg Am. 1953; 35:26–47. passim.
Article15. Guhl JF. Arthroscopic treatment of osteochondritis dissecans. Clin Orthop Relat Res. 1982; 167:65–74.
Article16. Dervin GF, Keene GC, Chissell HR. Biodegradable rods in adult osteochondritis dissecans of the knee. Clin Orthop Relat Res. 1998; 356:213–221.
Article17. Slough JA, Noto AM, Schmidt TL. Tibial cortical bone peg fixation in osteochondritis dissecans of the knee. Clin Orthop Relat Res. 1991; 267:122–127.
Article18. Smillie IS. Treatment of osteochondritis dissecans. J Bone Joint Surg Br. 1957; 39:248–260.
Article19. Thomson NL. Osteochondritis dissecans and osteochondral fragments managed by Herbert compression screw fixation. Clin Orthop Relat Res. 1987; 224:71–78.
Article20. Tuompo P, Arvela V, Partio EK, Rokkanen P. Osteochondritis dissecans of the knee fixed with biodegradable self-reinforced polyglycolide and polylactide rods in 24 patients. Int Orthop. 1997; 21:355–360.
Article21. Victoroff BN, Marcus RE, Deutsch A. Arthroscopic bone peg fixation in the treatment of osteochondritis dissecans in the knee. Arthroscopy. 1996; 12:506–509.
Article22. Ziran B, Marcus R. Biologic fixation of osteochondritis dissecans of the knee. Orthopaedics (International Edition). 1994; 2:527–532.23. Johnson LL, Uitvlugt G, Austin MD, Detrisac DA, Johnson C. Osteochondritis dissecans of the knee: arthroscopic compression screw fixation. Arthroscopy. 1990; 6:179–189.
Article24. Friederichs MG, Greis PE, Burks RT. Pitfalls associated with fixation of osteochondritis dissecans fragments using bioabsorbable screws. Arthroscopy. 2001; 17:542–545.
Article25. Hangody L, Karpati Z, Toth J, Dioszegi Z, Kendik Z, Bely M. Transplantation of osteochondral autografts of the weightbearing surface of the knee joint and the patellofemoral joint in dogs. Hung Rev Sports Med. 1994; 35:117–123.26. Yoshizumi Y, Sugita T, Kawamata T, Ohnuma M, Maeda S. Cylindrical osteochondral graft for osteochondritis dissecans of the knee: a report of three cases. Am J Sports Med. 2002; 30:441–445.27. Ahmad CS, Guiney WB, Drinkwater CJ. Evaluation of donor site intrinsic healing response in autologous osteochondral grafting of the knee. Arthroscopy. 2002; 18:95–98.
Article28. Sgaglione NA, Miniaci A, Gillogly SD, Carter TR. Update on advanced surgical techniques in the treatment of traumatic focal articular cartilage lesions in the knee. Arthroscopy. 2002; 18:2 Suppl 1. 9–32.
Article29. Gudas R, Kalesinskas RJ, Kimtys V, et al. A prospective randomized clinical study of mosaic osteochondral autologous transplantation versus microfracture for the treatment of osteochondral defects in the knee joint in young athletes. Arthroscopy. 2005; 21:1066–1075.
Article30. Duchow J, Hess T, Kohn D. Primary stability of press-fit-implanted osteochondral grafts. Influence of graft size, repeated insertion, and harvesting technique. Am J Sports Med. 2000; 28:24–27.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Concomitant Osteochondral Autograft Transplantation and Fixation of Osteochondral Fragment for Treatment of a Massive Osteochondritis Dissecans: A Report of 8-Year Follow-up Results
- Bilateral Osteochondritis Dissecans of the Femoral Condyles in Both Knees: A Report of Two Sibling Cases
- Autologous Osteochondral Transplantation as a Secondary Procedure after Failed Microfracture for Osteochondral Lesion of Talus
- Radiologic findings of osteochondritis dissecans
- Osteochondral Lesion of the Tibial Plafond: A Case Report
