Accessory Cardiac Bronchus: Proposed Imaging Classification on Multidetector CT
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University College of Medicine, Cheonan Hospital, Cheonan, Korea. ytokim@schmc.ac.kr
- KMID: 2152599
- DOI: http://doi.org/10.3348/jksr.2016.74.2.82
Abstract
- PURPOSE
To propose the classification of accessory cardiac bronchus (ACB) based on imaging using multidetector computed tomography (MDCT), and evaluate follow-up changes of ACB.
MATERIALS AND METHODS
This study included 58 patients diagnosed as ACB since 9 years, using MDCT. We analyzed the types, division locations and division directions of ACB, and also evaluated changes on follow-up.
RESULTS
We identified two main types of ACB: blind-end (51.7%) and lobule (48.3%). The blind-end ACB was further classified into three subtypes: blunt (70%), pointy (23.3%) and saccular (6.7%). The lobule ACB was also further classified into three subtypes: complete (46.4%), incomplete (28.6%) and rudimentary (25%). Division location to the upper half bronchus intermedius (79.3%) and medial direction (60.3%) were the most common in all patients. The difference in division direction was statistically significant between the blind-end and lobule types (p = 0.019). Peribronchial soft tissue was found in five cases. One calcification case was identified in the lobule type. During follow-up, ACB had disappeared in two cases of the blind-end type and in one case of the rudimentary subtype.
CONCLUSION
The proposed classification of ACB based on imaging, and the follow-up CT, helped us to understand the various imaging features of ACB.
Figure
-

Fig. 1 Schematic diagram of the proposed imaging classification of accessory cardiac bronchus, based on multidetector CT. Blind-end type is subclassified into blunt (Ia), pointy (Ib), and saccular (Ic) subtypes, according to the shape of the distal end of accessory cardiac bronchus. Lobule type is subclassfied into complete, incomplete and rudimentary subtypes. The complete subtype of lobule type (IIa) is defined as an accessory lobule with lung parenchyma (*) formed by the complete fissure (solid line). In the incomplete subtype of lobule type (IIb), accessory cardiac bronchus and lung parenchyma (*) form an incomplete lobule with/without a fissure-like structure (dashed line). In the rudimentary subtype of lobule type (IIc), accessory cardiac bronchus is not blinded, and is connected to an anomalous or vestigial lobule (dots).
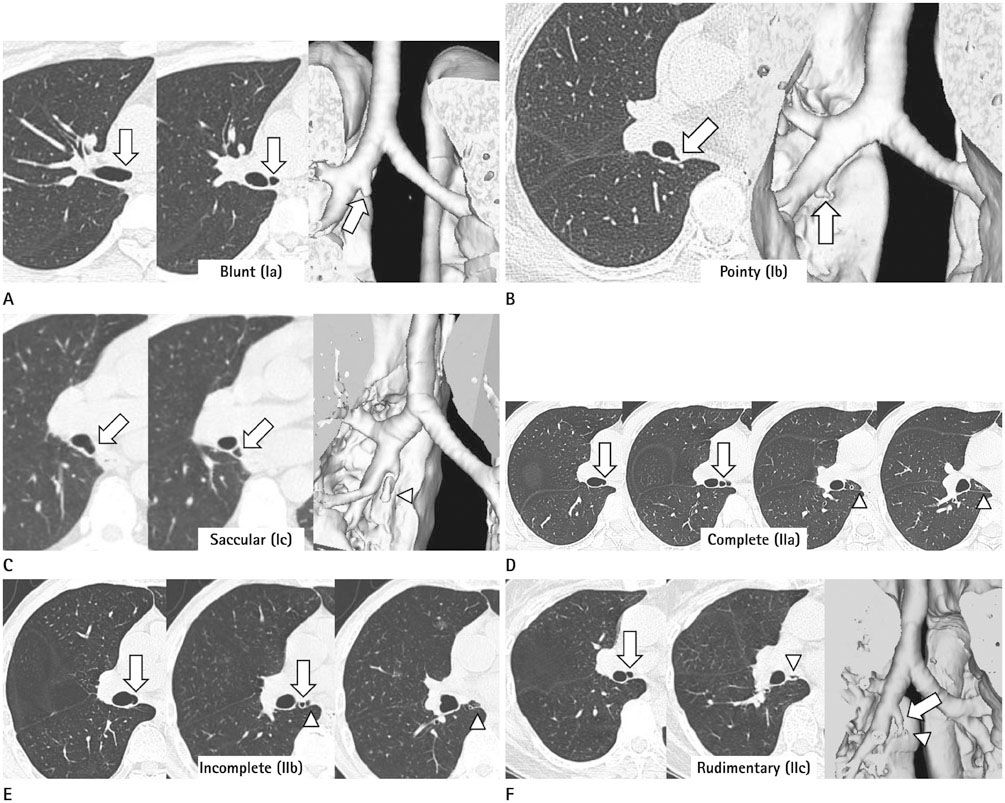
Fig. 2 The CT findings of accessory cardiac bronchus by imaging classification. A. Blunt subtype (Ia) of blind-end type in a 42-year-old woman. Axial and three dimensional images show the rounded-end of accessory cardiac bronchus (arrow), originating from the right main bronchus on the medial axis. B. Pointy subtype (Ib) of blind-end type in a 61-year-old woman. Axial and three dimensional images show the pointy shaped end of accessory cardiac bronchus (arrow), originating from the lower half of bronchus intermedius on the posteromedial axis. C. Saccular subtype (Ic) of blind-end type in a 60-year-old man. Axial images show the accessory cardiac bronchus (arrow), originating from the bronchus intermedius on the posteromedial axis. Three dimensional image shows a sac like structure (arrowhead) of the distal portion of accessory cardiac bronchus. D. Complete subtype (IIa) of lobule type in a 45-year-old man. Serial axial images show the accessory cardiac bronchus (arrow), originating from the bronchus intermedius on the medial axis. The accessory cardiac bronchus and surrounding lung parenchyma are separated from the right lower lobe by a complete anomalous fissure (arrowhead), forming an accessory lobule. E. Incomplete subtype (IIb) of lobule type and in a 70-year-old man. Serial axial images show the accessory cardiac bronchus (arrow) and a fissure-like structure (arrowhead). However, the lobule is not completely formed. F. Rudimentary subtype (IIc) of lobule type in a 60-year-old woman. Axial and three dimensional images show an irregularly shaped lobulus without lung parenchyma (arrowhead), distal to the accessory cardiac bronchus (arrow).
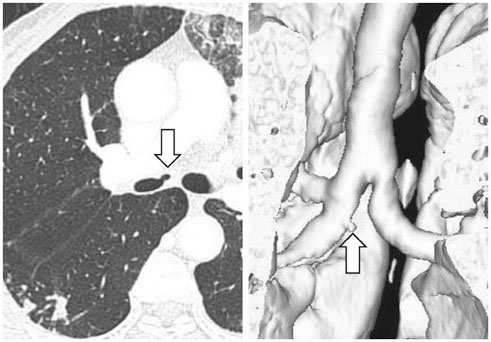
Fig. 3 The accessory cardiac bronchus with anteromedial direction, in a 69-year-old woman. Axial and three dimensional images show a small sized accessory cardiac bronchus (arrow) on anteromedial direction, originating from the upper half of intermedius bronchus.
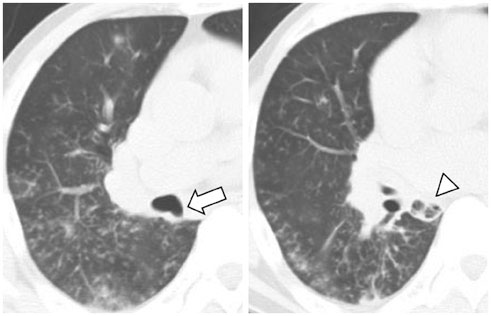
Fig. 4 The accessory cardiac bronchus with combined infection, in a 42-year-old man. Axial images show an accessory cardiac bronchus (arrow). Dirty increased opacities in an anomalous lobule (arrowhead) and thickening of an anomalous fissure, suggest inflammation. Pneumonia in the right lung supports this interpretation.

Fig. 5 Multiple small calcifications in an accessory cardiac bronchus, in a 71-year-old man. Serial axial images show an accessory cardiac bronchus (arrow) and multiple small calcifications in an anomalous lobule (arrowhead).

Fig. 6 A small vessel near the complete lobe of accessory cardiac bronchus, in a 57-year-old man. On contiguous axial CT images, a small vein (arrow) is positioned anterior to the complete lobe of accessory cardiac bronchus (asterisk), draining into the left atrium (LA).
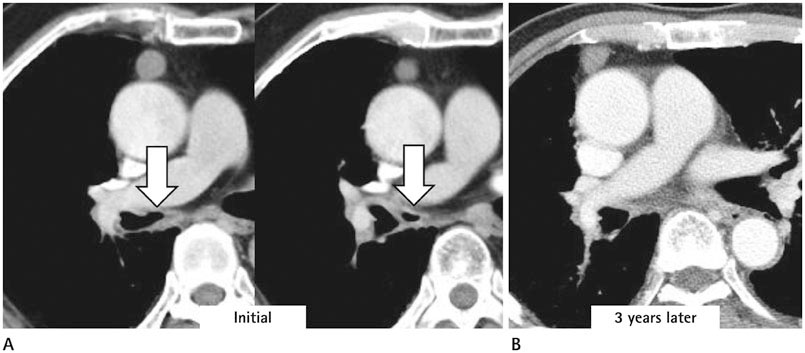
Fig. 7 The change in the shape of accessory cardiac bronchus in a 76-year-old man. A. Axial images show an irregularly shaped accessory cardiac bronchus (arrow) surrounded by soft tissue attenuation. B. CT scan, obtained after three years, shows that the accessory bronchus is obliterated.
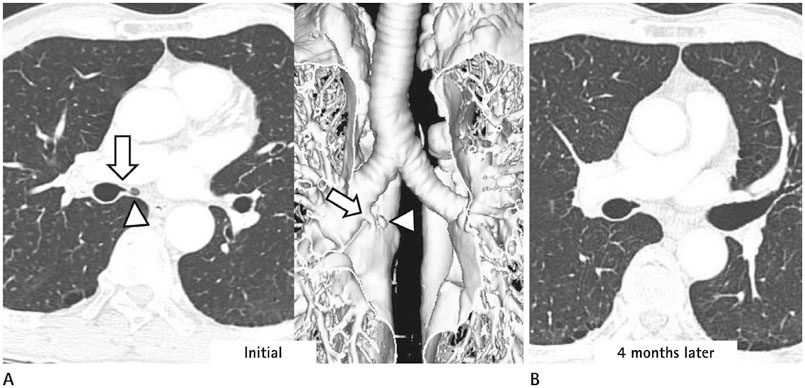
Fig. 8 The change in the shape of accessory cardiac bronchus in a 71-year-old woman. A. Axial and three dimensional images show an irregularly shaped lobulus (arrowhead) at the left side of the accessory cardiac bronchus (arrow). The cardiac bronchus is classified as rudimentary subtype (IIc) of lobule type. B. CT scan obtained after four months shows that the rudimentary lobule is obliterated.
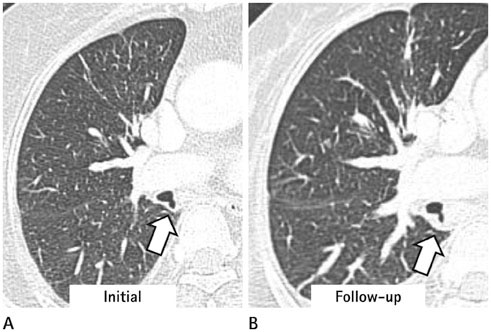
Fig. 9 The follow-up change of peribronchial soft tissue lesion in a 57-year-old woman with an accessory cardiac bronchus. A. An axial image shows thin peribronchial soft tissue lesion (arrow) at the wall of the accessory cardiac bronchus. The accessory cardiac bronchus was classified as blunt subtype (Ia) of blind-end type. B. The axial image obtained after six months shows the thickened peribronchial soft tissue lesion (arrow). There is no change in the shape of the accessory cardiac bronchus.
Reference
-
1. Brock RC. The anatomy of the bronchial tree. London: UK: Oxford University Press;1947.2. Zylak CJ, Eyler WR, Spizarny DL, Stone CH. Developmental lung anomalies in the adult: radiologic-pathologic correlation. Radiographics. 2002; 22 Spec No:S25–S43.3. Chung S, Shim YM. Accessory cardiac bronchus with lung cancer: a case report. Korean J Thorac Cardiovasc Surg. 2010; 43:550–552.4. Miyahara R, Hasegawa S, Yoshimura T, Wada H. A case of squamous cell carcinoma arising from accessory cardiac bronchus. Eur J Cardiothorac Surg. 2002; 22:309.5. Dunnick NR. Image interpretation session: 1999. Accessory cardiac bronchus. Radiographics. 2000; 20:264–225.6. Bentala M, Grijm K, van der Zee JH, Kloek JJ. Cardiac bronchus: a rare cause of hemoptysis. Eur J Cardiothorac Surg. 2002; 22:643–645.7. Ghaye B, Kos X, Dondelinger RF. Accessory cardiac bronchus: 3D CT demonstration in nine cases. Eur Radiol. 1999; 9:45–48.8. Endo S, Saitoh N, Murayama F, Sohara Y, Fuse K. Symptomatic accessory cardiac bronchus. Ann Thorac Surg. 2000; 69:262–264.9. Katayama K, Tsuyuguchi M, Hino N, Okada M, Haku T, Kiyoku H. Adult case of accessory cardiac bronchus presenting with bloody sputum. Jpn J Thorac Cardiovasc Surg. 2005; 53:641–644.10. Sotile SC, Brady MB, Brogdon BG. Accessory cardiac bronchus: demonstration by computed tomography. J Comput Tomogr. 1988; 12:144–146.11. Suzuki M, Matsui O, Takemura A, Kobayashi T, Yoneda K, Shibata Y. Four cases of accessory cardiac bronchus incidentally detected on multi-detector CT. Eur J Radiol Extra. 2006; 57:47–50.12. Ghaye B, Szapiro D, Fanchamps JM, Dondelinger RF. Congenital bronchial abnormalities revisited. Radiographics. 2001; 21:105–119.13. Atwell SW. Major anomalies of the tracheobronchial tree: with a list of the minor anomalies. Dis Chest. 1967; 52:611–615.14. Atwell SW. An aberrant bronchus. Ann Thorac Surg. 1966; 2:438–441.15. Mangiulea VG, Stinghe RV. The accessory cardiac bronchus. Bronchologic aspect and review of the literature. Dis Chest. 1968; 54:433–436.16. McGuinness G, Naidich DP, Garay SM, Davis AL, Boyd AD, Mizrachi HH. Accessory cardiac bronchus: CT features and clinical significance. Radiology. 1993; 189:563–566.17. Shtasel P, Jordan L. The accessory cardiac bronchial stump: case reports. J Am Osteopath Assoc. 1966; 65:486–469.18. Zanetti G, Hochhegger B, Guimarães MD, Marchiori E. Accessory cardiac bronchus causing recurrent pulmonary infection. J Bras Pneumol. 2014; 40:448–449.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Accessory Cardiac Bronchus with Lung Cancer: A case report
- CT-Based Essential Cardiac Anatomy for Radiology Residents to Understand Congenital Heart Disease
- True Tracheal Bronchus: Classification and Anatomical Relationship on Multi-Detector Computed Tomography
- Myocardial Contractility, Perfusion, and Viability Analysis Using Multidetector CT in Patients with Ischemic Heart Disease
- Coronary Angiography with Multidetector row Computed Tomography: Part I - Technical Aspects
