True Tracheal Bronchus: Classification and Anatomical Relationship on Multi-Detector Computed Tomography
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. ytokim@schmc.ac.kr
- KMID: 2373963
- DOI: http://doi.org/10.3348/jksr.2017.76.4.264
Abstract
- PURPOSE
To propose the imaging classification of true tracheal bronchus (TTB) on multi-detector computed tomography (MDCT), and to evaluate its anatomical relationship with surrounding structures.
MATERIALS AND METHODS
This study included 44 patients who were diagnosed with TTB on MDCT for 6 years. We classified TTB into five types, based on the existence of the right upper lobe bronchus originating from the right main bronchus and the number of segmental bronchi of TTB. We analyzed the site of origin and the running direction of TTB based on its anatomical relationship with surrounding structures and some ancillary findings.
RESULTS
The imaging classification of TTB included Type I (47.7%), Type II (13.6%), Type III (11.4%), Type IV (25.0%), and Type V (2.0%). According to the site of origin of TTB, below the aortic arch (52.3%) and at the level of the aortic arch (43.1%) were the two main sites of origin, whereas the frequency of the site of origin above the azygos arch, at the level of the azygos arch, and below the azygos arch was 27.3%, 38.6%, and 34.1%, respectively. Considering both aortic and azygos arches, below the aortic arch and below the azygos arch were the most common sites of origin (27.3%). With respect to the running direction of TTB, in all cases, TTB passed below the azygos arch to the right upper lobe. There was no statistically significant (p > 0.05) difference in age or sex between types of TTB. Ancillary findings included tracheal stenosis (n = 2), narrowing of the right main bronchus (n = 2), luminal narrowing of TTB and bronchiectasis at the distal portion (n = 1), and a highly located azygos arch above the aortic arch (n = 2).
CONCLUSION
The proposed imaging classification of TTB and its anatomical relationship with surrounding structures will improve our understanding of various imaging features and embryological development of TTB. Radiologists should pay careful attention to evaluation of the airway including the trachea on thoracic imaging.
MeSH Terms
Figure
-
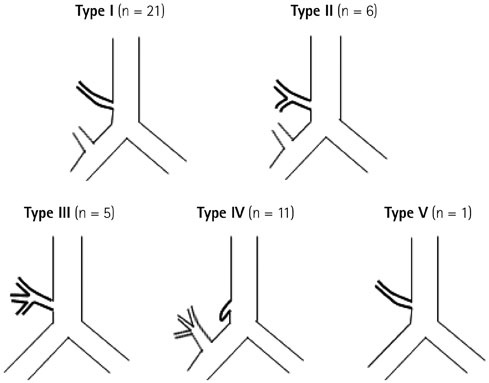
Fig. 1 Imaging classification of true tracheal bronchus on MDCT. Type I: Anomalous one segmental bronchus arising from the lower trachea to the right upper lobe with existence of the right upper lobe bronchus originating from the main bronchus. Type II: Anomalous two segmental bronchi arising from the lower trachea to the right upper lobe with existence of the right upper lobe bronchus originating from the main bronchus. Type III: The entire right upper lobe bronchus arising from the lower trachea without existence of the right upper lobe bronchus arising from the main bronchus. Type IV: Anomalous bronchus arising from the lower trachea with a blind end. Type V: Anomalous segmental bronchus arising from the lower trachea to the right upper lobe without existence of the right upper lobe bronchus arising from the main bronchus. MDCT = multi-detector computed tomography
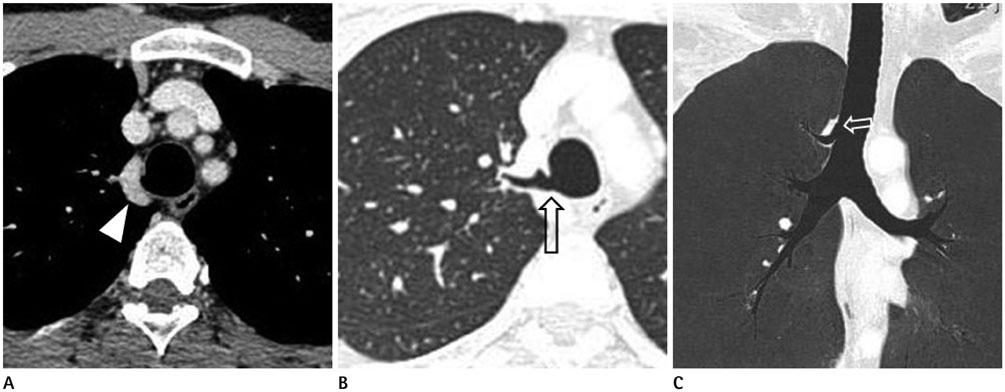
Fig. 2 True tracheal bronchus (Type I) in an asymptomatic 35-year-old man. A. Axial CT image showing a highly located azygos arch (arrowhead) at the level of site of origin of thoracic great vessels. B, C. Axial CT (B) and coronal minimum intensity projection (C) images showing true tracheal bronchus (open arrow) originating at the level of the azygos arch and running below the azygos arch.
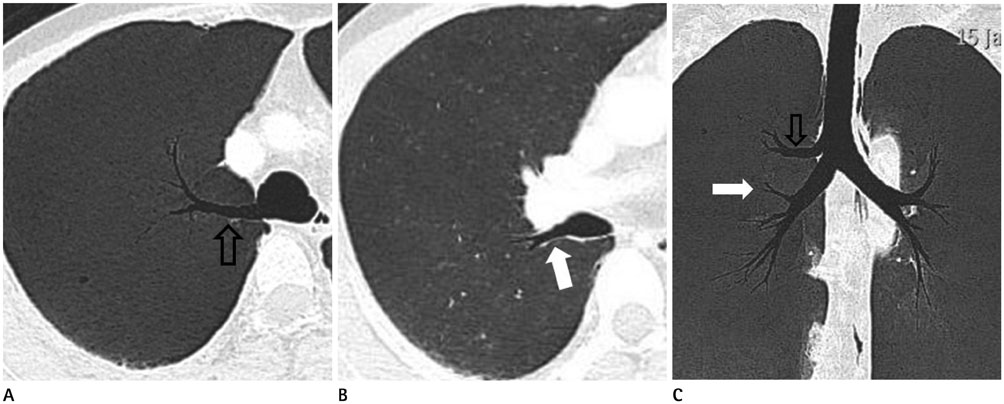
Fig. 3 True tracheal bronchus (Type II) in an asymptomatic 37-year-old man. Axial (A, B) and coronal minimum intensity projection (C) images showing anomalous two segmental bronchi (open arrow in A, C) arising from the lower trachea and one segmental bronchus (solid arrow in B, C) arising from the distal portion of the right main bronchus.

Fig. 4 True tracheal bronchus (Type III) in a 49-year-old man with chronic cough and dyspnea. Coronal volume rendering (A) and minimum intensity projection (B) images showing an entire right upper lobe bronchus (open arrow) originating from the lower trachea. The lower trachea distal to the origin of tracheal bronchus is markedly narrowed. The diameter of the right main bronchus is less than or equal to that of the left main bronchus.
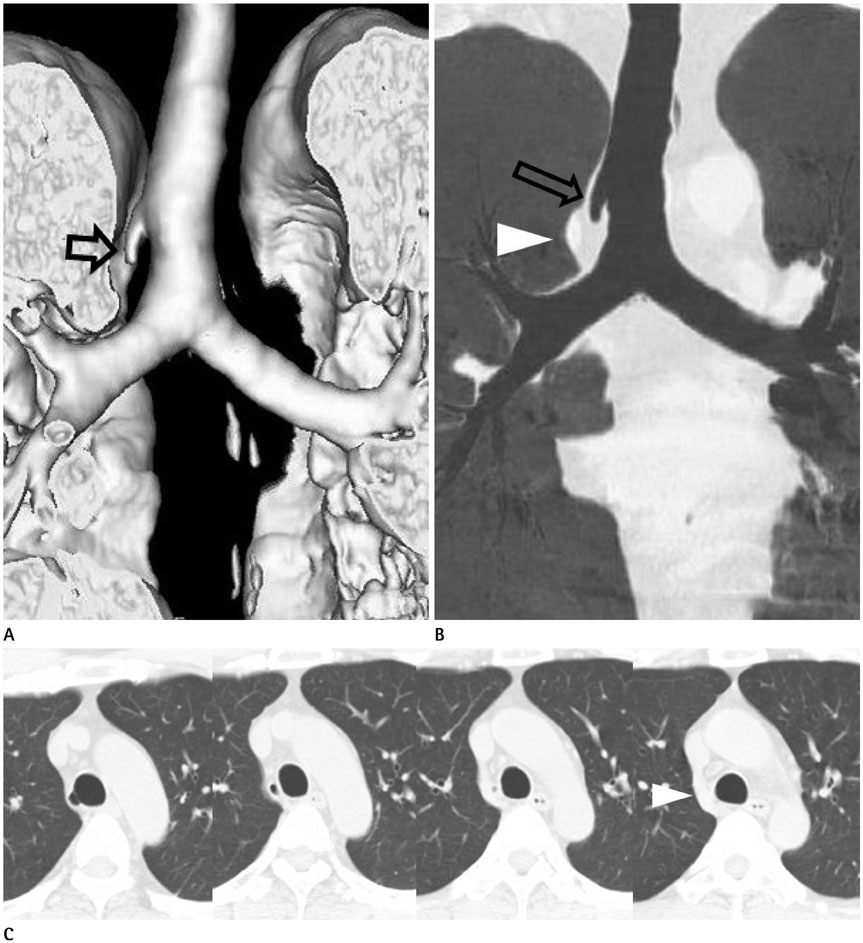
Fig. 5 True tracheal bronchus (Type IV) in an asymptomatic 53-year-old man. Coronal volume rendering (A) and minimum intensity projection (MinIP, B) images showing an anomalous bronchus with a blind end (open arrow), arising from the lower trachea. It is also called tracheal diverticulum. On coronal MinIP (B) and serial axial CT (C) images, true tracheal bronchus ends blindly within the mediastinal fat, medial to the azygos arch (arrowhead).
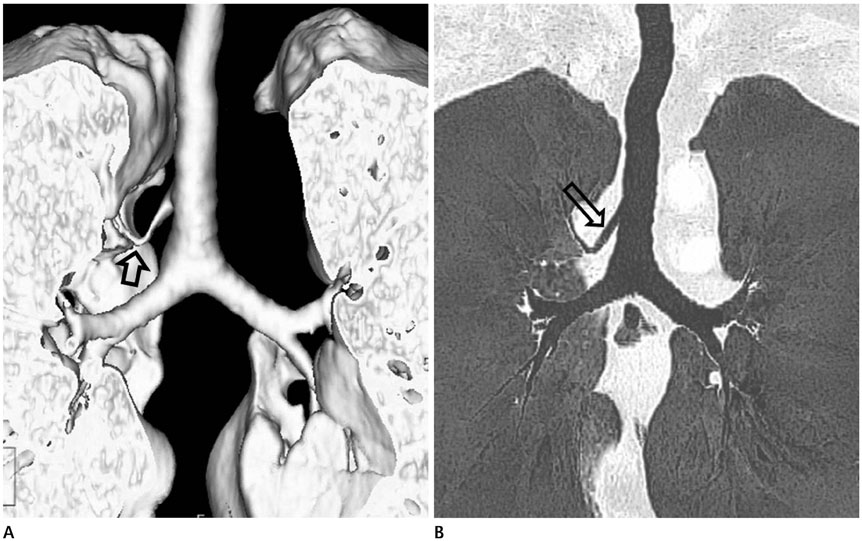
Fig. 6 True tracheal bronchus (Type V) in a 71-year-old man with chronic cough. Coronal volume rendering (A) and minimum intensity projection (B) images showing an anomalous segmental bronchus (open arrow) arising from the lower trachea without existence of the right upper lobe bronchus arising from the right main bronchus. The diameter of the right main bronchus is less than that of the left main bronchus.
Reference
-
1. Ghaye B, Szapiro D, Fanchamps JM, Dondelinger RF. Congenital bronchial abnormalities revisited. Radiographics. 2001; 21:105–119.2. Ming Z, Lin Z. Evaluation of tracheal bronchus in Chinese children using multidetector CT. Pediatr Radiol. 2007; 37:1230–1234.3. Suzuki M, Matsui O, Kawashima H, Takemura A, Matsubara K, Hayashi N, et al. Radioanatomical study of a true tracheal bronchus using multidetector computed tomography. Jpn J Radiol. 2010; 28:188–192.4. Hong MJ, Kim YT, Jou SS, Park AY. Tracheobronchial branching anomalies. J Korean Soc Radiol. 2010; 63:149–159.5. Doolittle AM, Mair EA. Tracheal bronchus: classification, endoscopic analysis, and airway management. Otolaryngol Head Neck Surg. 2002; 126:240–243.6. Ulusoy M, Kivrak AS, Uysal II, Karabulut AK, Paksoy Y, Fazliogullari Z. Developmental anomalies of bronchial tree: a multidetector computerized tomography study. Int J Morphol. 2013; 31:1049–1055.7. Barat M, Konrad HR. Tracheal bronchus. Am J Otolaryngol. 1987; 8:118–122.8. Jou SS, Kim YT, Bae WK, Kim IY, Kim HH, Han JK. Evaluation of tracheal and main bronchial diverticula using thin-section MDCT. J Korean Soc Radiol. 2010; 62:123–130.9. Beigelman C, Howarth NR, Chartrand-Lefebvre C, Grenier P. Congenital anomalies of tracheobronchial branching patterns: spiral CT aspects in adults. Eur Radiol. 1998; 8:79–85.10. Gonlugur U, Efeoglu T, Kaptanoglu M, Akkurt I. Major anatomical variations of the tracheobronchial tree: bronchoscopic observation. Anat Sci Int. 2005; 80:111–115.11. Miabi Z, Alaee A, Midia M, Hashemi H. Detection of rare congenital tracheal anomalies by multidetector CT in an infant. Acta Med Iran. 2006; 44:429–431.12. Ritsema GH. Ectopic right bronchus: indication for bronchography. AJR Am J Roentgenol. 1983; 140:671–674.13. Lee DK, Kim YM, Kim HZ, Lim SH. Right upper lobe tracheal bronchus: anesthetic challenge in one-lung ventilated patients -A report of three cases-. Korean J Anesthesiol. 2013; 64:448–450.14. Bremer JL. Accessory bronchi in embryos; their occurrence and probable fate. Anat Rec. 1932; 54:361–374.15. Reid L. 1976 Edward B.D. Neuhauser lecture: the lung: growth and remodeling in health and disease. AJR Am J Roentgenol. 1977; 129:777–788.16. Alescio T, Cassini A. Induction in vitro of tracheal buds by pulmonary mesenchyme grafted on tracheal epithelium. J Exp Zool. 1962; 150:83–94.17. Gower WA, McGrath-Morrow SA, MacDonald KD, Fishman EK. Tracheal bronchus in a 6-month-old infant identified by CT with three-dimensional airway reconstruction. Thorax. 2008; 63:93–94.18. Buterbaugh JE, Erly WK. Paratracheal air cysts: a common finding on routine CT examinations of the cervical spine and neck that may mimic pneumomediastinum in patients with traumatic injuries. AJNR Am J Neuroradiol. 2008; 29:1218–1221.19. Kosehan D, Kayıhan A, Koktener A. Incidental right paratracheal air cyst: significance of 64-detector multislice CT in differential diagnosis. New J Med. 2011; 28:62–63.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Demonhstration of a Tracheal Bronchus by Bronchoscopy and Computed Tompgraphy
- A Case of Displaced Lobar Tracheal Bronchus Associated with Bronchiectasis
- A Case of Tracheal Bronchus
- The Clinical Consideration of Tracheal Bronchus Detected by Computed Tomography Scan in Children
- The EZ-Blocker® for one-lung ventilation in a patient with Kartagener syndrome and tracheal bronchus -a case report-
