The Clinical Utility of FDG PET-CT in Evaluation of Bone Marrow Involvement by Lymphoma
- Affiliations
-
- 1Department of Internal Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea. hemonc@hallym.or.kr
- 2Department of Laboratory Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- 3Department of Pathology, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- 4Department of Nuclear Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea. hshwang@hallym.or.kr
- 5Department of Preventive Medicine, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2148495
- DOI: http://doi.org/10.4143/crt.2014.091
Abstract
- PURPOSE
Bone marrow biopsy is a standard method for the evaluation of bone marrow infiltration by lymphoma; however, it is an invasive and painful procedure. Fluorodeoxyglucose positron emission tomography-computed tomography (FDG PET-CT) is a noninvasive imaging technique with the potential to detect bone marrow involvement by lymphoma.
MATERIALS AND METHODS
We retrospectively reviewed medical records of lymphoma patients. All patients were examined by FDG PET-CT and iliac crest bone marrow biopsy for initial staging work-up.
RESULTS
The study population comprised 94 patients (median age, 60 years; 56 males) with Hodgkin's lymphoma (n=8) or non-Hodgkin's lymphoma (n=86). Maximum standardized uptake values on the iliac crest of patients with lymphoma infiltrated bone marrow were significantly higher than those of patients with intact bone marrow (2.2+/-1.2 g/mL vs. 1.3+/-0.4 g/mL; p=0.001). The calculated values for FDG PET-CT during evaluation of bone marrow involvement were as follows: sensitivity 50%, specificity 96%, positive predictive value 80%, negative predictive value 85%, and positive likelihood ratio (LR+) 11.7. The value of LR+ was 16.0 in patients with aggressive subtypes of non-Hodgkin's lymphoma (NHL).
CONCLUSION
FDG PET-CT could not replace bone marrow biopsy due to the low sensitivity of FDG PET-CT for detection of bone marrow infiltration in lymphoma patients. Conversely, FDG PET-CT had high specificity and LR+; therefore, it could be a useful tool for image-guided biopsy for lymphoma staging, especially for aggressive subtypes of NHL. In addition, unilateral bone marrow biopsy could be substituted for bilateral bone marrow biopsy in lymphoma patients with increased FDG uptake on any iliac crest.
MeSH Terms
Figure
-
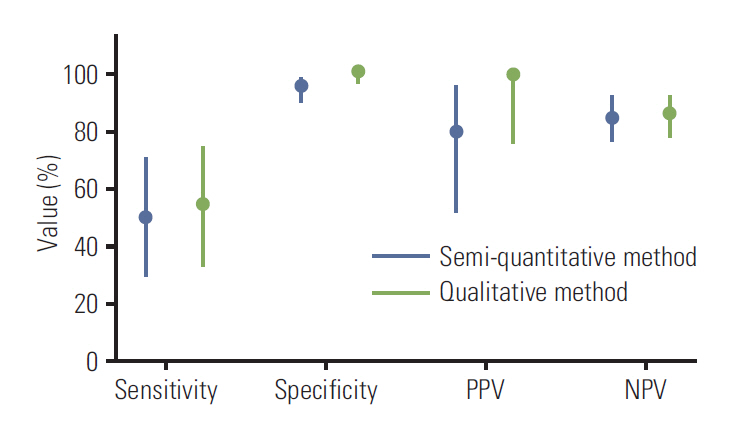
Fig. 1. Comparison of the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of fluorodeoxyglucose positron emission tomography– computed tomography during detection of bone marrow involvement between the semi-quantitative and qualitative method; 95% confidence intervals are displayed as a line.
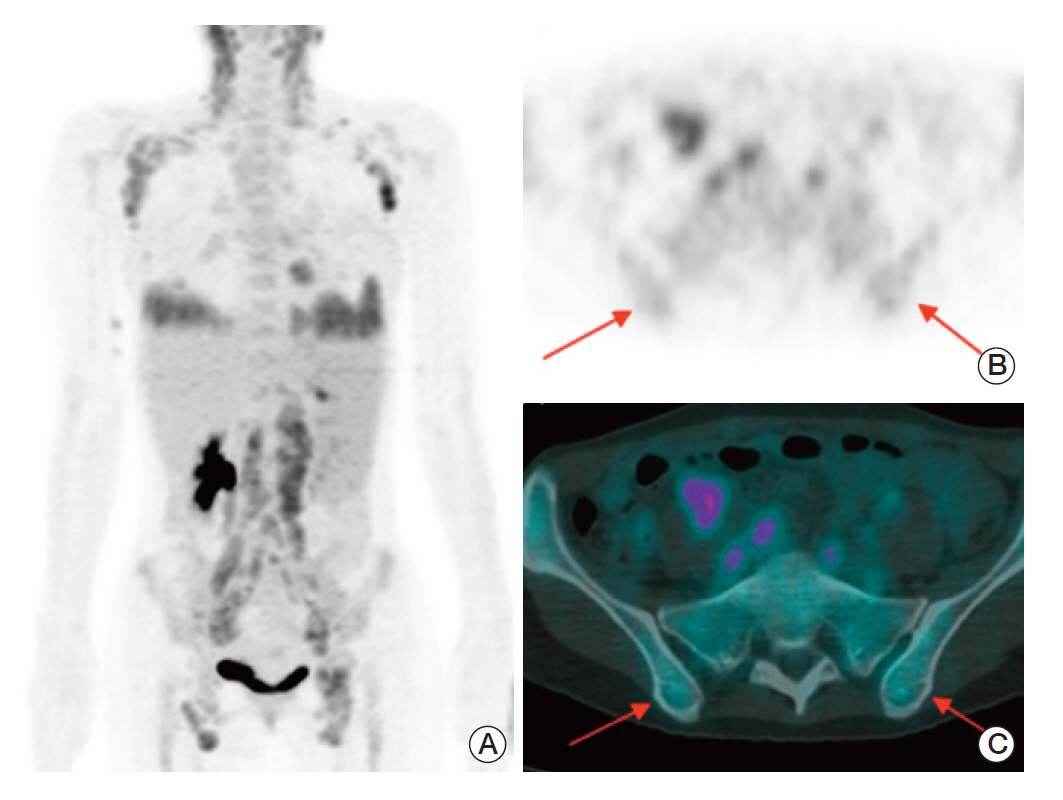
Fig. 2. A 40-year-old female patient with angioimmunoblastic T-cell lymphoma. (A) Maximum intensity projection of positron emission tomography–computed tomography (PET-CT) shows multiple enlarged lymph nodes with increased fluorodeoxyglucose (FDG) uptake in the bilateral neck, axillar, retroperitoneal, iliac, and inguinal areas. Increased FDG uptakes in both lower lung fields suggest lung involvement. Transaxial PET (B) and fusion PET-CT (C) images demonstrate mild increased FDG uptake in bone marrow of iliac crests (arrows). The maximum standardized uptake value at the posterior iliac crest is 2.2 g/mL on the right and 2.4 g/mL on the left, respectively.
Reference
-
References
1. Jost LM, Stahel RA; ESMO Guidelines Task Force. ESMO Minimum clinical recommendations for diagnosis, treatment and follow-up of Hodgkin's disease. Ann Oncol. 2005; 16 Suppl 1:i54–5.
Article2. Hiddemann W, Dreyling M, Stahel RA; ESMO Guidelines Task Force. Minimum clinical recommendations for diagnosis, treatment and follow-up of newly diagnosed follicular lymphoma. Ann Oncol. 2005; 16 Suppl 1:i56–7.
Article3. Zhang QY, Foucar K. Bone marrow involvement by Hodgkin and non-Hodgkin lymphomas. Hematol Oncol Clin North Am. 2009; 23:873–902.
Article4. Juneja SK, Wolf MM, Cooper IA. Value of bilateral bone marrow biopsy specimens in non-Hodgkin's lymphoma. J Clin Pathol. 1990; 43:630–2.
Article5. Gronich N, Radnay J, Shapiro H, Manor Y, Lahav M, Lishner M. Clinical outcome of low-grade NHL patients with bone marrow involvement. Eur J Clin Invest. 2007; 37:305–9.
Article6. Sasaki M, Kuwabara Y, Koga H, Nakagawa M, Chen T, Kaneko K, et al. Clinical impact of whole body FDG-PET on the staging and therapeutic decision making for malignant lymphoma. Ann Nucl Med. 2002; 16:337–45.
Article7. Muslimani AA, Farag HL, Francis S, Spiro TP, Chaudhry AA, Chan VC, et al. The utility of 18-F-fluorodeoxyglucose positron emission tomography in evaluation of bone marrow involvement by non-Hodgkin lymphoma. Am J Clin Oncol. 2008; 31:409–12.
Article8. Schaefer NG, Strobel K, Taverna C, Hany TF. Bone involvement in patients with lymphoma: the role of FDG-PET/CT. Eur J Nucl Med Mol Imaging. 2007; 34:60–7.
Article9. Khan AB, Barrington SF, Mikhaeel NG, Hunt AA, Cameron L, Morris T, et al. PET-CT staging of DLBCL accurately identifies and provides new insight into the clinical significance of bone marrow involvement. Blood. 2013; 122:61–7.
Article10. Pelosi E, Penna D, Deandreis D, Chiappella A, Skanjeti A, Vitolo U, et al. FDG-PET in the detection of bone marrow disease in Hodgkin's disease and aggressive non-Hodgkin's lymphoma and its impact on clinical management. Q J Nucl Med Mol Imaging. 2008; 52:9–16.11. Chen YK, Yeh CL, Tsui CC, Liang JA, Chen JH, Kao CH. F-18 FDG PET for evaluation of bone marrow involvement in non-Hodgkin lymphoma: a meta-analysis. Clin Nucl Med. 2011; 36:553–9.12. Brunning RD, Bloomfield CD, McKenna RW, Peterson LA. Bilateral trephine bone marrow biopsies in lymphoma and other neoplastic diseases. Ann Intern Med. 1975; 82:365–6.
Article13. Coller BS, Chabner BA, Gralnick HR. Frequencies and patterns of bone marrow involvement in non-Hodgkin lymphomas: observations on the value of bilateral biopsies. Am J Hematol. 1977; 3:105–19.
Article14. Malempati S, Joshi S, Lai S, Braner DA, Tegtmeyer K. Videos in clinical medicine: bone marrow aspiration and biopsy. N Engl J Med. 2009; 361:e28.15. Arellano-Rodrigo E, Real MI, Muntanola A, Burrel M, Rozman M, Fraire GV, et al. Successful treatment by selective arterial embolization of severe retroperitoneal hemorrhage secondary to bone marrow biopsy in post-polycythemic myelofibrosis. Ann Hematol. 2004; 83:67–70.
Article16. Moog F, Bangerter M, Kotzerke J, Guhlmann A, Frickhofen N, Reske SN. 18-F-fluorodeoxyglucose-positron emission tomography as a new approach to detect lymphomatous bone marrow. J Clin Oncol. 1998; 16:603–9.
Article17. Carr R, Barrington SF, Madan B, O'Doherty MJ, Saunders CA, van der Walt J, et al. Detection of lymphoma in bone marrow by whole-body positron emission tomography. Blood. 1998; 91:3340–6.
Article18. Campbell JK, Matthews JP, Seymour JF, Wolf MM, Juneja SK; Australasian Leukaemia Lymphoma Group. Optimum trephine length in the assessment of bone marrow involvement in patients with diffuse large cell lymphoma. Ann Oncol. 2003; 14:273–6.
Article19. Conlan MG, Bast M, Armitage JO, Weisenburger DD. Bone marrow involvement by non-Hodgkin's lymphoma: the clinical significance of morphologic discordance between the lymph node and bone marrow. Nebraska Lymphoma Study Group. J Clin Oncol. 1990; 8:1163–72.
Article20. Bennett JM, Cain KC, Glick JH, Johnson GJ, Ezdinli E, O'Connell MJ. The significance of bone marrow involvement in non-Hodgkin's lymphoma: the Eastern Cooperative Oncology Group experience. J Clin Oncol. 1986; 4:1462–9.
Article21. Kang YK, Kim BS, Kim TW, Ryu MH, Lee SS, Ryoo BY, et al. Clinicopathologic charcteristics of Korean non-Hodgkin's lymphomas based on REAL classification. J Korean Cancer Assoc. 1999; 31:641–52.22. Okada J, Yoshikawa K, Itami M, Imaseki K, Uno K, Itami J, et al. Positron emission tomography using fluorine-18-fluorodeoxyglucose in malignant lymphoma: a comparison with proliferative activity. J Nucl Med. 1992; 33:325–9.23. Goldberg MA, Lee MJ, Fischman AJ, Mueller PR, Alpert NM, Thrall JH. Fluorodeoxyglucose PET of abdominal and pelvic neoplasms: potential role in oncologic imaging. Radiographics. 1993; 13:1047–62.
Article24. Pakos EE, Fotopoulos AD, Ioannidis JP. 18F-FDG PET for evaluation of bone marrow infiltration in staging of lymphoma: a meta-analysis. J Nucl Med. 2005; 46:958–63.25. Divgi C. Imaging: staging and evaluation of lymphoma using nuclear medicine. Semin Oncol. 2005; 32(1 Suppl 1):S11–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of 18F-FDG PET/CT for the Evaluation of Bone Marrow Involvement in Patients with High-Grade Non-Hodgkin's Lymphoma
- Detection of bone marrow involvement with FDG PET/CT in patients with newly diagnosed lymphoma
- Staging and response assessment of lymphoma: a brief review of the Lugano classification and the role of FDG-PET/CT
- Prognostic Value of Bone Marrow F-18 FDG Uptake in Patients with Advanced-Stage Diffuse Large B-Cell Lymphoma
- Diffuse Bone Marrow Uptake of 99mTc-MIBI in A Case of Intravascular Large B-cell Lymphoma
