Ann Rehabil Med.
2015 Aug;39(4):649-653. 10.5535/arm.2015.39.4.649.
Lumbar Epidural Steroid Injection for Painful Spasticity in Cervical Spinal Cord Injury: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul, Korea. keewonkimm.d@gmail.com
- KMID: 2148239
- DOI: http://doi.org/10.5535/arm.2015.39.4.649
Abstract
- We report a case of a 53-year-old male with traumatic cervical spinal cord injury (SCI). He could not maintain a standing position because of painful spasticity in his lower limbs. A magnetic resonance imaging and electromyography indicated chronic lumbosacral radiculopathy, explaining his chronic low back pain before the injury. For diagnostic as well as therapeutic purposes, transforaminal epidural steroid injection (ESI) to the right L5 root was performed. After the intervention, the spasticity decreased and his ambulatory function improved. This case illustrates that lumbar radiculopathy concomitant with a cervical SCI can produce severe spasticity and it can be dramatically improved by ESI.
MeSH Terms
Figure
-
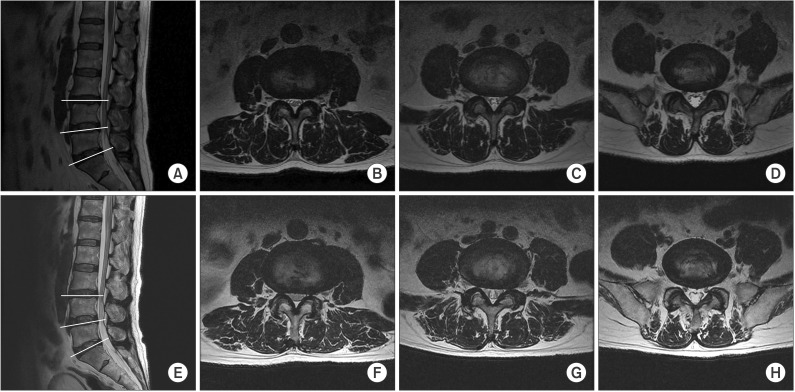
Fig. 1 T2-weighted magnetic resonance imaging of the lumbar spine. (A-D) About 1 year before the injury. (A) Mid-sagittal view. (B) Axial view at L3/4 level. (C) Axial view at L4/5 level. (D) Axial view at L5/S1 level. (E-H) After the cord injury. (E) Mid-sagittal view. (F) Axial view at L3/4 level. (G) Axial view at L4/5 level. (H) Axial view at L5/S1 level.
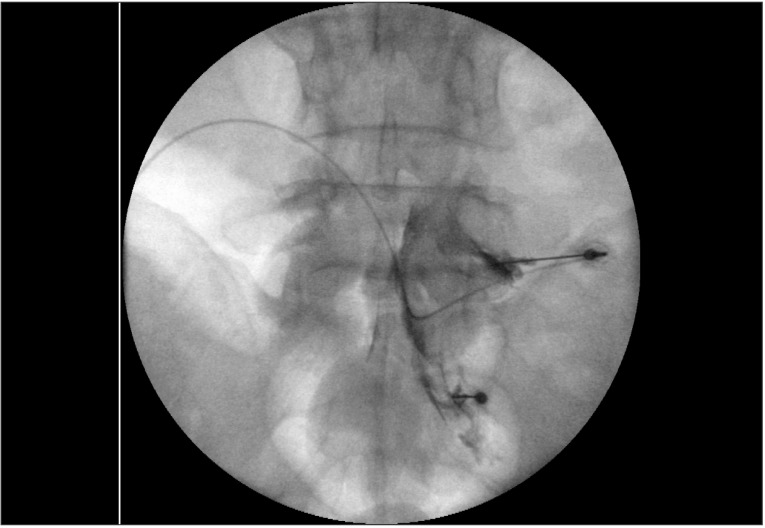
Fig. 2 Right L5 transforaminal epidural steroid injection under fluoroscopic guidance. Injection level was determined by symptom provocation with 0.9% normal saline at L5 and S1 levels.
Reference
-
1. Adams MM, Hicks AL. Spasticity after spinal cord injury. Spinal Cord. 2005; 43:577–586.
Article2. Rekand T, Hagen EM, Gronning M. Spasticity following spinal cord injury. Tidsskr Nor Laegeforen. 2012; 132:970–973. PMID: 22562332.3. Han IH, Suh SH, Kuh SU, Chin DK, Kim KS. Types and prevalence of coexisting spine lesions on whole spine sagittal MR images in surgical degenerative spinal diseases. Yonsei Med J. 2010; 51:414–420. PMID: 20376895.
Article4. LaBan MM, Green ML. Concurrent (tandem) cervical and lumbar spinal stenosis: a 10-yr review of 54 hospitalized patients. Am J Phys Med Rehabil. 2004; 83:187–190. PMID: 15043352.5. Aydogan M, Ozturk C, Mirzanli C, Karatoprak O, Tezer M, Hamzaoglu A. Treatment approach in tandem (concurrent) cervical and lumbar spinal stenosis. Acta Orthop Belg. 2007; 73:234–237. PMID: 17515237.6. Takao T, Morishita Y, Okada S, Maeda T, Katoh F, Ueta T, et al. Clinical relationship between cervical spinal canal stenosis and traumatic cervical spinal cord injury without major fracture or dislocation. Eur Spine J. 2013; 22:2228–2231. PMID: 23793521.
Article7. Nakae R, Onda H, Yokobori S, Araki T, Fuse A, Toda S, et al. Clinical analysis of spinal cord injury with or without cervical ossification of the posterior longitudinal ligament, spondylosis, and canal stenosis in elderly head injury patients. Neurol Med Chir (Tokyo). 2010; 50:461–465. PMID: 20587969.
Article8. Regenbogen VS, Rogers LF, Atlas SW, Kim KS. Cervical spinal cord injuries in patients with cervical spondylosis. AJR Am J Roentgenol. 1986; 146:277–284. PMID: 3484576.
Article9. Akuthota V, Nadler SF. Core strengthening. Arch Phys Med Rehabil. 2004; 85(3 Suppl 1):S86–S92. PMID: 15034861.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Cervical Subdural Hematoma with Quadriparesis after Cervical Transforaminal Epidural Block
- Fibrous Mass Complicating Epidural Steroid and Local Anesthetic Injection: A Case Report
- Low Extremity Weakness after Cervical Epidural Steroid Injection in Previous Spinal Surgery Patient: A case report
- Accidental Subdural Injection during Attempted Cervical Epidural Block: Radiologic Evidence : A case report
- Lumbar Spinal Stenosis Induced by Epidural Lipomatosis: A case report
