Korean Circ J.
2010 Apr;40(4):197-200. 10.4070/kcj.2010.40.4.197.
Acute Myocardial Infarction due to Polyarteritis Nodosa in a Young Female Patient
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. ygko@yuhs.ac
- 2Division of Rheumatology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 3Division of Cardiology, Department of Internal Medicine, College of Medicine, Soonchunhyang University, Seoul, Korea.
- KMID: 2145557
- DOI: http://doi.org/10.4070/kcj.2010.40.4.197
Abstract
- Coronary artery aneurysms are uncommon, are usually associated with atherosclerosis, and rarely involve all three major coronary arteries. The present report describes a rare case of a young female patient presenting with acute myocardial infarction (AMI). Coronary angiography revealed multiple severe aneurysmal and stenotic changes. Based on clinical feature and angiographic findings, it was strongly suspected that the patient had polyarteritis nodosa (PAN) complicated by AMI. The patient was treated with standard cardiac medications and immunosuppressive agents and has remained stable without further complications during a follow-up period of 6 months.
MeSH Terms
Figure
-

Fig. 1 Coronary angiography. A: anteroposterior caudal view shows multiple aneurysmal changes of the left main and the left anterior descending artery with total occlusion of the left circumflex artery. B: left anterior oblique cranial view shows a huge aneurysmal dilatation of the proximal part and critical stenotic lesions of the posterolateral branch in the right coronary artery.
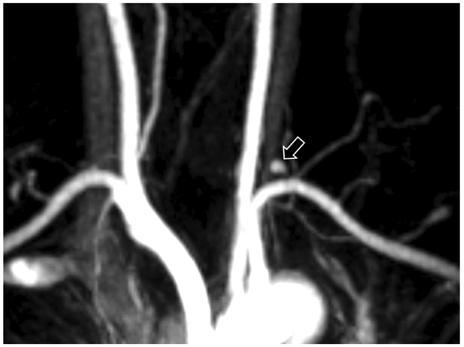
Fig. 2 Brain magnetic resonance angiography. A small aneurysm arose from the left thyrocervical trunk (arrow).

Fig. 3 Computed tomographic angiography. A small aneurysm was seen at the posterior division of the left renal artery (arrow).
Reference
-
1. Villines TC, Avedissian LS, Elgin EE. Diffuse nonatherosclerotic coronary aneurysms: an unusual cause of sudden death in a young male and a literature review. Cardiol Rev. 2005. 13:309–311.2. Mirza A. Myocardial infarction resulting from nonatherosclerotic coronary artery diseases. Am J Emerg Med. 2003. 21:578–584.3. Swaye PS, Fisher LD, Litwin P, et al. Aneurysmal coronary artery disease. Circulation. 1983. 67:134–138.4. Chia HM, Tan KH, Jackson G. Non-atherosclerotic coronary artery aneurysms: two case reports. Heart. 1997. 78:613–616.5. Kabaoğlu B, Coşkun H, Yanar H, Karaarslan E, Yalti T. A rare case of splenic infarct presenting with acute abdominal pain due to polyarteritis nodosa: case report and review of the literature. Ulus Travma Acil Cerrahi Derg. 2005. 11:242–246.6. Yun HJ, Kim KS, Hur SH, Park NH, Cho YW. A case report of a huge coronary artery aneurysm with acute myocardial infarction. Korean Circ J. 2002. 32:720–724.7. Desai PK, Ro JH, Pucillo A, Weiss MB, Herman MV. Left main coronary artery aneurysm following percutaneous transluminal angioplasty: a report of a case and review of the literature. Cathet Cardiovasc Diagn. 1992. 27:113–116.8. Chu KH, Menapace FJ, Blankenship JC, Hausch R, Harrington T. Polyarteritis nodosa presenting as acute myocardial infarction with coronary dissection. Cathet Cardiovasc Diagn. 1998. 44:320–324.9. Lightfoot RW Jr, Michel BA, Bloch DA, et al. The American College of Rheumatology 1990 criteria for the classification of polyarteritis nodosa. Arthritis Rheum. 1990. 33:1088–1093.10. Gayraud M, Guillevin L, le Toumelin P, et al. Long-term follow-up of polyarteritis nodosa, microscopic polyangiitis, and Churg-Strauss syndrome: analysis of four prospective trials including 278 patients. Arthritis Rheum. 2001. 44:666–675.11. Guillevin L, Lhote F, Cohen P, et al. Corticosteroids plus pulse cyclophosphamide and plasma exchanges versus corticosteroids plus pulse cyclophosphamide alone in the treatment of polyarteritis nodosa and Churg-Strauss syndrome patients with factors predicting poor prognosis: a prospective, randomized trial in sixty-two patients. Arthritis Rheum. 1995. 38:1638–1645.12. Choi HJ, Jung SA, Lee EY, Jung HK, Shin GJ, Lee WH. A case of polyarteritis nodosa combined with dilated cardiomyopathy. Korean Circ J. 1994. 24:668–674.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Spontaneous Repture of Renal Artery Aneurysm in Polyarteritis Nodosa
- Ischemic Pseudomembranous Colitis with Perforation due to Polyarteritis Nodosa
- A Case of Polyarteritis Nodosa Presented as Myositis
- Polyarteritis Nodosa Presenting as Acute Myocardial Infarction
- A case of polyarteritis nodosa complicated by bilateral renal hematomas and U.G.I. bleeding
