Infectious Spondylitis Mimicking Osteoporotic Vertebral Compression Fractures: Report of Two Cases
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea Cancer Center Hospital, Seoul, Korea.
- 2Department of Orthopedic Surgery, Seoul National University College of Medicine, Seoul, Korea. bschang@snu.ac.kr
- KMID: 2144774
- DOI: http://doi.org/10.4184/jkss.2014.21.3.123
Abstract
- STUDY DESIGN: Case study of two cases.
OBJECTIVES
The aim of our study is to describe the rare MR imaging patterns of infectious spondylitis. SUMMARY OF LITERATURE REVIEW: It is generally accepted that the intravertebral cleft sign is not shown in cases of infection or malignancy, and thus, its recognition can obviate unnecessary imaging or biopsy because of its benign significance.
MATERIALS AND METHODS
Two patients are presented who developed worsening back pain after a minor trauma. Preoperative MR images of these patients showed intravertebral fluid and benign vertebral compression fractures. Anterior decompression and fusion were done and the bacteria isolated from the intraoperative cultures were Listeria monocytogenes and Mycobacterium tuberculosis, respectively.
RESULTS
After 2 years of follow-up, the patients were free of pain, without signs of infection, and showed correct fusion.
CONCLUSIONS
MR findings in infectious spondylitis may simulate the patterns of osteoporotic VCFs.
Keyword
MeSH Terms
Figure
-

Fig. 1. Sagittal CT and MR images of a 73-year-old woman who developed low back pain after slip down injury. She was thought to have osteoporotic vertebral compression fracture. However, CRP and blood cultures indicated a vertebral osteomyelitis, which was confirmed by open bone biopsy. (A) Lateral radiograph shows a compression fracture of L3 (B) Sagittal CT demonstrates the intravertebral cleft sign in the body of L3. (C) T1-weighted image (620/13) shows diminished height of the L3 vertebral body. (D) T2-weighted image (4000/114) shows intravertebral fluid and a minimal amount of epidural inflammatory tissue at the L3 level, which were initially interpreted as hematoma. (E) T1-weighted fat-suppressed contrast-enhanced image (639/15) shows marginal enhancement of the vertebral body.
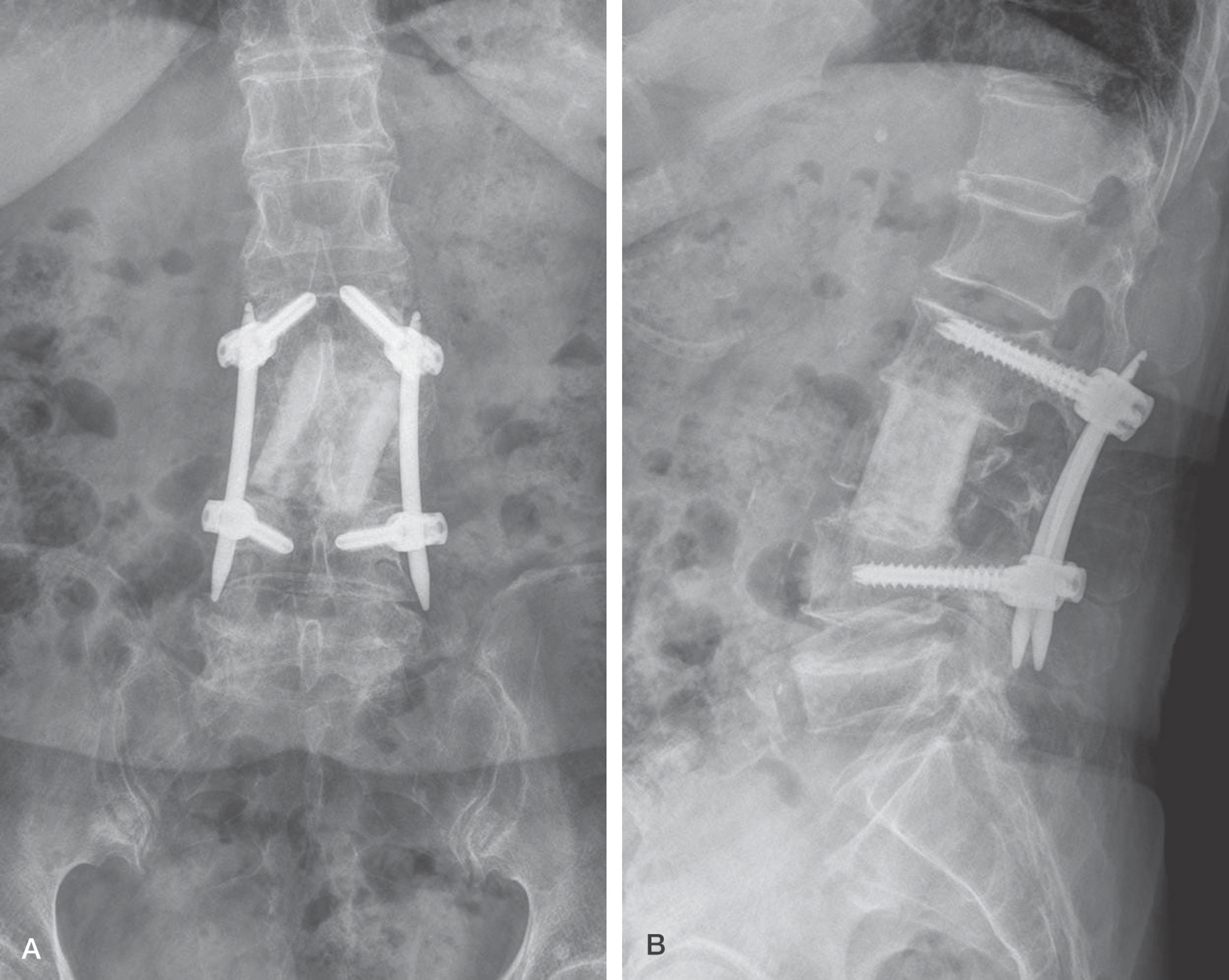
Fig. 2. (A) AP and (B) lateral radiographs which were taken after 2 years of followup show a solid bony fusion.
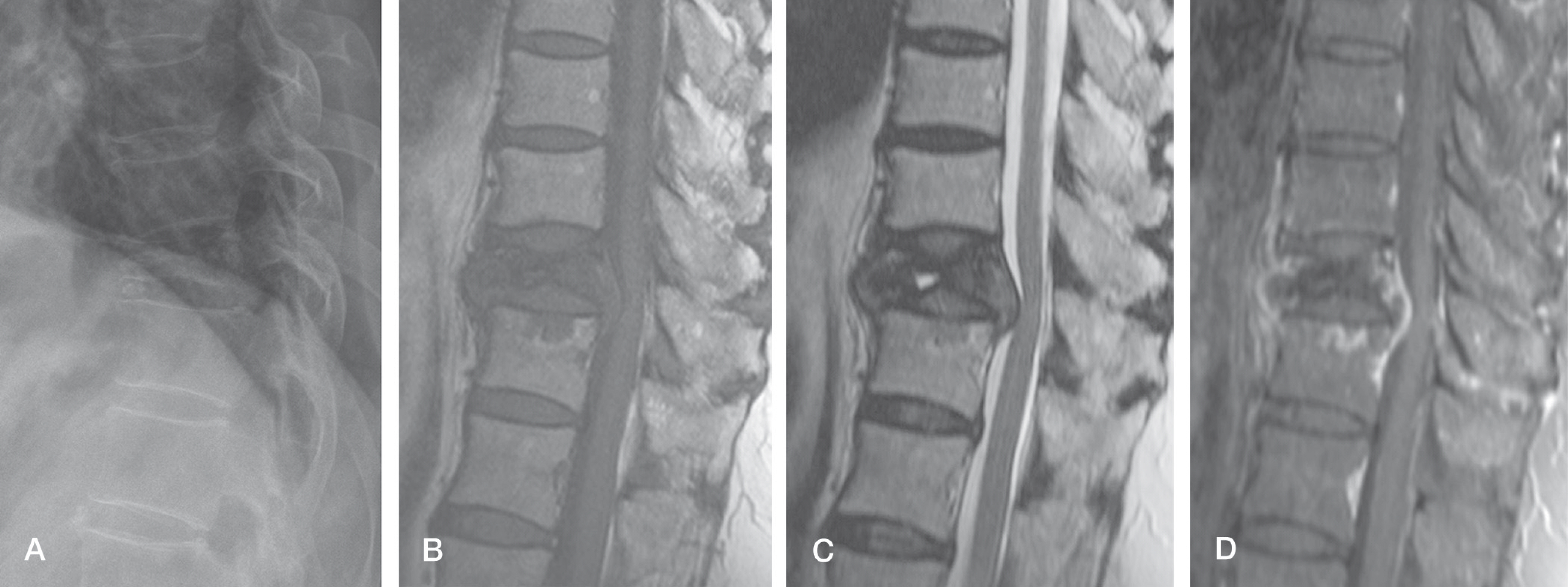
Fig. 3. Lateral radiograph and sagittal MR images of T10 vertebral lesion simulating osteoporotic vertebral compression fracture in a 61-year-old woman who suffered from chronic back pain without any trauma history. She was initially thought to have the typical Kümmell's disease, but her final diagnosis was tuberculous spondylitis. (A) Radiograph shows severe vertebral collapse of the T10 vertebra. Note that standing lateral radiograph makes T10 vertebra more kyphotic comparing to MR images. (B) T1-weighted image (550/13) shows diminished height of the T10 vertebral body. (C) T2-weighted image (4000/101) shows intravertebral fluid and mild cord compression. (D) T1-weighted fat-suppressed contrast-enhanced image (664/13) shows marginal enhancement of the vertebral body.
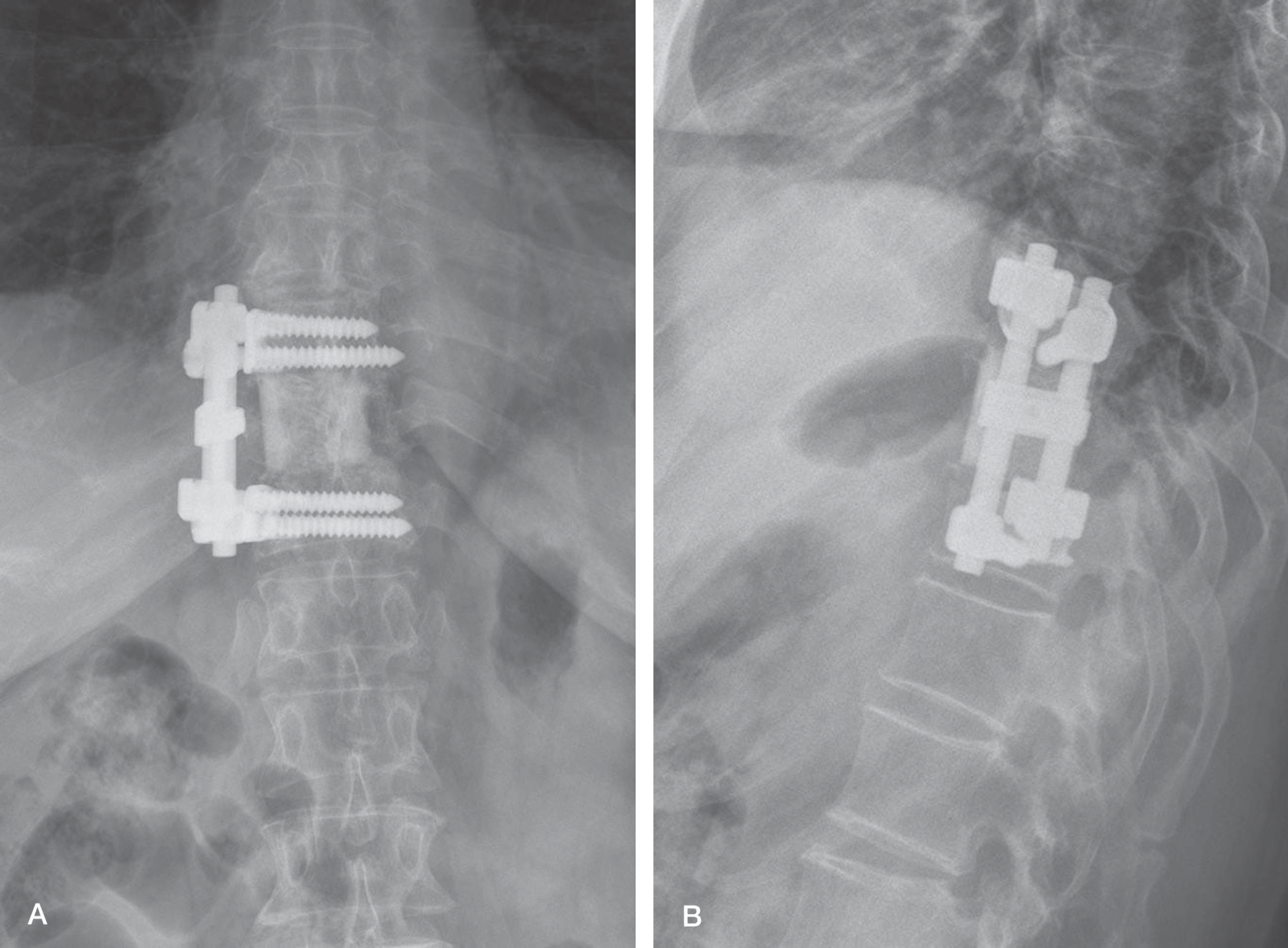
Fig. 4. (A) AP and (B) lateral radiographs which were taken after 2 years of followup show a solid bony fusion.
Reference
-
1. Ledermann HP, Schweitzer ME, Morrison WB, Carrino JA. MR imaging findings in spinal infections: rules or myths? Radiology. 2003; 228:506–14.
Article2. Bhalla S, Reinus WR. The linear intravertebral vacuum: a sign of benign vertebral collapse. AJR Am J Roentgenol. 1998; 170:1563–9.
Article3. Yu SW, Chen WJ, Lin WC, Chen YJ, Tu YK. Serious pyogenic spondylitis following vertebroplasty–a case report. Spine. 2004; 29:E209–11.
Article4. Pande KC, Babhulkar SS. Atypical spinal tuberculosis. Clin Orthop Relat Res. 2002; 398:67–74.
Article5. Thrush A, Enzmann D. MR imaging of infectious spondylitis. AJNR Am J Neuroradiol. 1990; 11:1171–80.6. Gillams AR, Chaddha B, Carter AP. MR appearances of the temporal evolution and resolution of infectious spondylitis. AJR Am J Roentgenol. 1996; 166:903–07.
Article7. Bouvresse S, Chiras J, Bricaire F, Bossi P. Pott's disease oc-curring after percutaneous vertebroplasty: an unusual illus-tration of the principle of locus minoris resistentiae. J Infect. 2006; 53:E251–3.
Article8. Maldague BE, Noel HM, Malghem JJ. The intravertebral vacuum cleft: a sign of ischemic vertebral collapse. Radiology. 1978; 129:23–9.
Article9. Baur A, Stabler A, Arbogast S, Duerr HR, Bartl R, Reiser M. Acute osteoporotic and neoplastic vertebral compression fractures: fluid sign at MR imaging. Radiology. 2002; 225:730–5.
Article10. Bielecki DK, Sartoris D, Resnick D, Van Lom K, Fierer J, Haghighi P. Intraosseous and intradiscal gas in association with spinal infection: report of three cases. AJR Am J Roentgenol. 1986; 147:83–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vertebroplasty in the Multiple Osteoporotic Compression Fracture
- Pyogenic Spondylitis after Vertebroplasty: A Report of Two Cases
- Osteoporotic Lumbar Compression Fracture in Patient with Ankylosing Spondylitis Treated with Kyphoplasty
- Spontaneous Height Restoration of Vertebral Compression Fracture: A Case Report
- Vertebral compression fractures: distinction between benign and malignant causes with Tc-99m labeled antigranulocyte antibody immunoscintigraphy
