Temporomandibular joint involvement in malignant otitis externa: a case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, National Health Insurance Corporation Ilsan Hospital, Goyang, Korea. ilsanoms@gmail.com
- KMID: 2136994
- DOI: http://doi.org/10.5125/jkaoms.2011.37.6.535
Abstract
- Malignant otitis externa (MOE) originates as inflammation of the epidermis in the external auditory canal, and spreads to the surrounding structures and neck, leading to abscess formation. MOE is associated with an immunosuppressive condition and diabetes. Patients with MOE suffer from otalgia, otorrhea and hearing loss. According to the literature, surgery to the temporomandibular joint is controversial as the treatment of choice.
Keyword
MeSH Terms
Figure
-
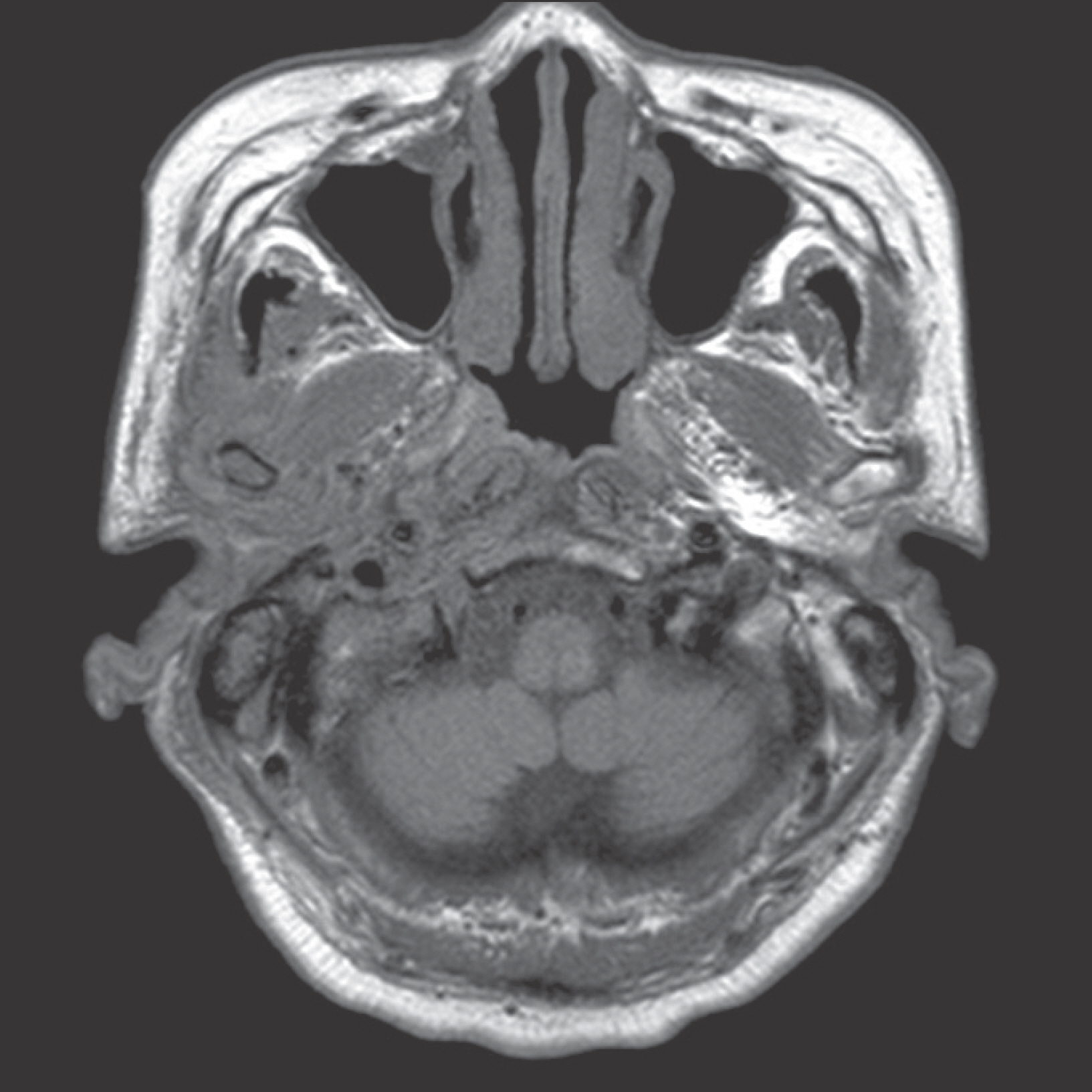
Fig. 1. Preoperative T1-weighted magnetic resonance image (MRI). MRI shows thick soft tissue surrounding right condylar head. In-Young Byun et al: Temporomandibular joint involvement in malignant otitis externa: a case report. J Korean Assoc Oral Maxillofac Surg 2011

Fig. 2. Preoperative T2-weighted magnetic resonance image. Right mastoid air cells were filled with fluid contents (arrows). In-Young Byun et al: Temporomandibular joint involvement in malignant otitis externa: a case report. J Korean Assoc Oral Maxillofac Surg 2011
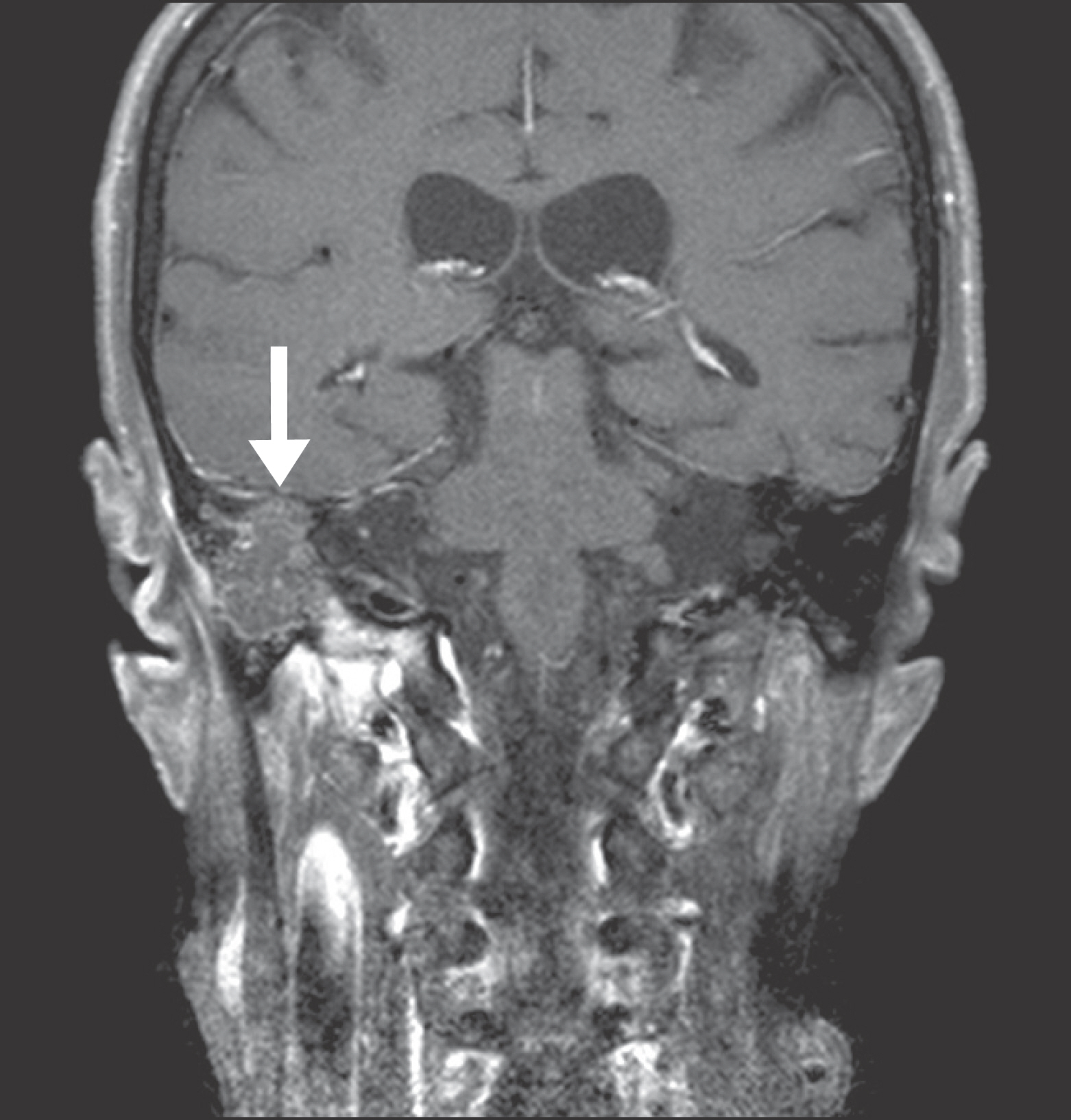
Fig. 3. Preoperative gadolinium-enhanced magnetic resonance image. Mass-like lesion (arrow) in right temporal bone invaded skull base. In-Young Byun et al: Temporomandibular joint involvement in malignant otitis externa: a case report. J Korean Assoc Oral Maxillofac Surg 2011

Fig. 4. Preoperative panoramic image. Cortical discontinuity in posterior border of right condylar head was note (arrow). In-Young Byun et al: Temporomandibular joint involvement in malignant otitis externa: a case report. J Korean Assoc Oral Maxillofac Surg 2011

Fig. 5. Preoperative temporomandibular joint magnetic resonance images. A. Left temporomandibular joint: normal structure. B. Right temporomandibular joint: joint cavity was filled with thick soft tissue (arrows). In-Young Byun et al: Temporomandibular joint involvement in malignant otitis externa: a case report. J Korean Assoc Oral Maxillofac Surg 2011
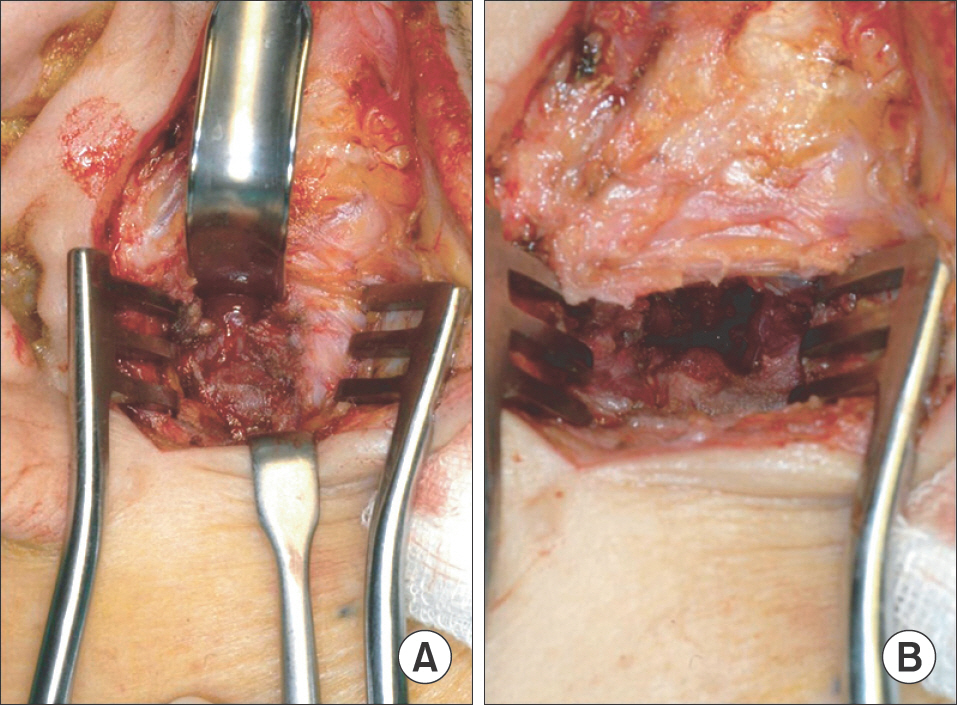
Fig. 6. Intraoperative photographs. A. Joint cavity was filled with inflammatory tissue. B. After inflammatory tissue removal: posterior surface of the condylar head was eroded. In-Young Byun et al: Temporomandibular joint involvement in malignant otitis externa: a case report. J Korean Assoc Oral Maxillofac Surg 2011

Fig. 7. Postoperative T2-weighted magnetic resonance image. Mastoiditis (arrow) was newly developed in left mastoid air cell compared to previous study. In-Young Byun et al: Temporomandibular joint involvement in malignant otitis externa: a case report. J Korean Assoc Oral Maxillofac Surg 2011
Reference
-
References
1. Chandler JR. Malignant external otitis. Laryngoscope. 1968; 78:1257–94.
Article2. Nadol JB Jr. Histopathology of Pseudomonas osteomyelitis of the temporal bone starting as malignant external otitis. Am J Otolaryngol. 1980; 1:359–71.
Article3. Naghibi M, Smith RP, Baltch AL, Gates SA, Wu DH, Hammer MC, et al. The effect of diabetes mellitus on chemotactic and bactericidal activity of human polymorphonuclear leukocytes. Diabetes Res Clin Pract. 1987; 4:27–35.
Article4. Geerlings SE, Hoepelman AI. Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunol Med Microbiol. 1999; 26:259–65.
Article5. Driscoll PV, Ramachandrula A, Drezner DA, Hicks TA, Schaffer SR. Characteristics of cerumen in diabetic patients: a key to understanding malignant external otitis? Otolaryngol Head Neck Surg. 1993; 109:676–9.6. Slattery WH 3rd, Brackmann DE. Skull base osteomyelitis. Malignant external otitis. Otolaryngol Clin North Am. 1996; 29:795–806.7. Bernheim J, Sade J. Histopathology of the soft parts in 50 patients with malignant external otitis. J Laryngol Otol. 1989; 103:366–8.
Article8. Singh A, Al Khabori M, Hyder MJ. Skull base osteomyelitis: diagnostic and therapeutic challenges in atypical presentation. Otolaryngol Head Neck Surg. 2005; 133:121–5.
Article9. Narozny W, Kuczkowski J, Stankiewicz C, Kot J, Mikaszewski B, Przewozny T. Value of hyperbaric oxygen in bacterial and fungal malignant external otitis treatment. Eur Arch Otorhinolaryngol. 2006; 263:680–4.
Article10. Franco-Vidal V, Blanchet H, Bebear C, Dutronc H, Darrouzet V. Necrotizing external otitis: a report of 46 cases. Otol Neurotol. 2007; 28:771–3.11. Kwon BJ, Han MH, Oh SH, Song JJ, Chang KH. MRI findings and spreading patterns of necrotizing external otitis: is a poor outcome predictable? Clin Radiol. 2006; 61:495–504.
Article12. Babiatzki A, Sadé J. Malignant external otitis. J Laryngol Otol. 1987; 101:205–10.
Article13. Mardinger O, Rosen D, Minkow B, Tulzinsky Z, Ophir D, Hirshberg A. Temporomandibular joint involvement in malignant external otitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 96:398–403.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diseases of External Auditory Canal and Middle Ear Communicating with Temporomandibular Joint: 2 Case Reports
- Temporomandibular Joint Disorder from Skull Base Osteomyelitis: A Case Report
- The Difference of External Auditory Canal pH in 3 Groups of Otitis Externa
- Synchronous Occurrence of Bilateral Malignant Otitis Externa: Report of a Rare Case
- Temporomandibular joint disorder from skull-base osteomyelitis: a case report
