Ovarian Tumor-Associated Carcinoid Heart Disease Presenting as Severe Tricuspid Regurgitation
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Keimyung University Dongsan Medical Center, Daegu, Korea. khyungseop@dsmc.or.kr
- KMID: 2135434
- DOI: http://doi.org/10.4250/jcu.2011.19.1.45
Abstract
- Carcinoid heart disease is characterized by heart valve dysfunction as well as carcinoid symptomatology. We report a case of carcinoid heart disease associated with a primary ovarian tumor. A 60-year-old woman presented for dyspnea evaluation with a history of facial flushing, telangiectatic skin changes, and pitting edema of both lower extremities. Chest radiography showed cardiomegaly, and echocardiography revealed an isolated, severe tricuspid regurgitation without left-sided valvular dysfunction. The tricuspid leaflets were severely retracted and shortened, resulting in poor coaptation. Furthermore, mild pulmonary valve stenosis and moderate regurgitation were found along with this deformation. The 24-hour urine analysis revealed an increased level of 5-hydroxyindoleacetic acid, and an ovarian tumor was apparent on computed tomography images. The mass was surgically removed, and the patient was diagnosed as having a primary ovarian carcinoid tumor. She was treated with chemotherapy and regularly followed-up with supportive treatments, deferring surgical correction.
MeSH Terms
Figure
-
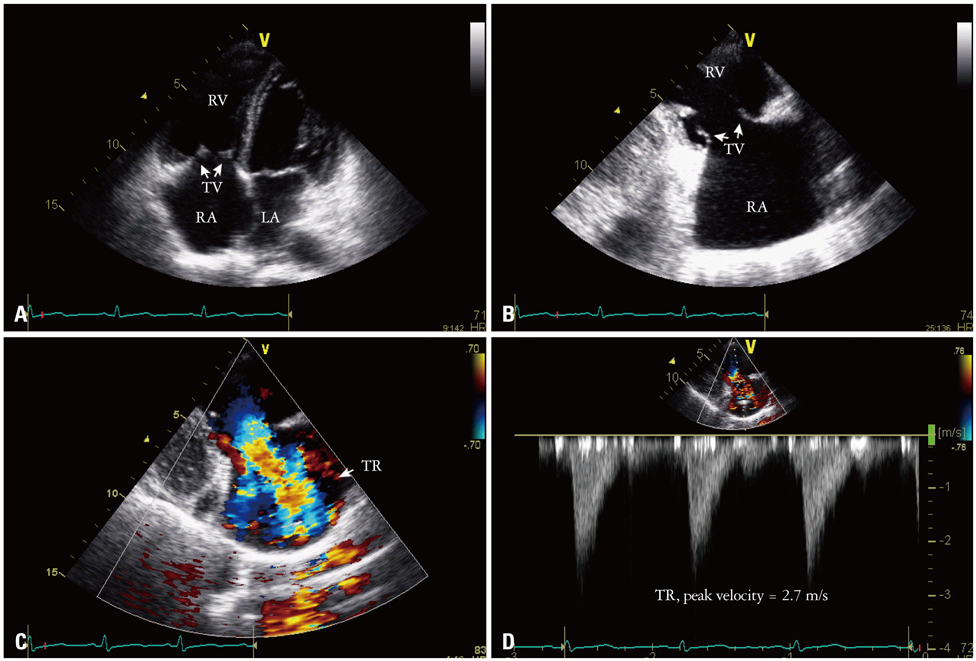
Fig. 1 Echocardiographic imagings showing a deformed tricuspid valve with regurgitation. The echocardiogram on apical four-chamber view shows an enlarged right atrium and right ventricle. Both anterior and septal leaflets (arrows) reveal thickened and retracted (A). On the right ventricular inflow view, both anterior and posterior leaflets also show no mobility, shortening, and coaptation failure (B). Severe tricuspid regurgitation is noted on color Doppler imaging (C). Continuous-wave Doppler signal of tricuspid regurgitation shows an early peak velocity and a rapid decline, shaping dagger-shaped "V" wave (velocity, 2.7 m/s) (D). RV: right ventricle, RA: right atrium, LA: left atrium, TV: tricuspid valve, TR: tricuspid regurgitation.

Fig. 2 Echocardiographic imagings showing a deformed pulmonary valve with regurgitation and stenosis. Parasternal short axis view of the pulmonary valve which has thickened and shortened leaflets (arrows); in addition, pulmonary annular contraction is present in zoomed imaging (A and D). On color Doppler imaging, moderate pulmonary regurgitation is shown and its peak velocity is at 1.5 m/s (B and C). Simultaneously, color flow is accelerated in systolic phase due to the stiffened and constricted leaflets (peak velocity, 1.8 m/s) (E and F). RV: right ventricle, Ao: aorta, PV: pulmonary valve, PR: pulmonary regurgitation, PS: pulmonary stenosis.
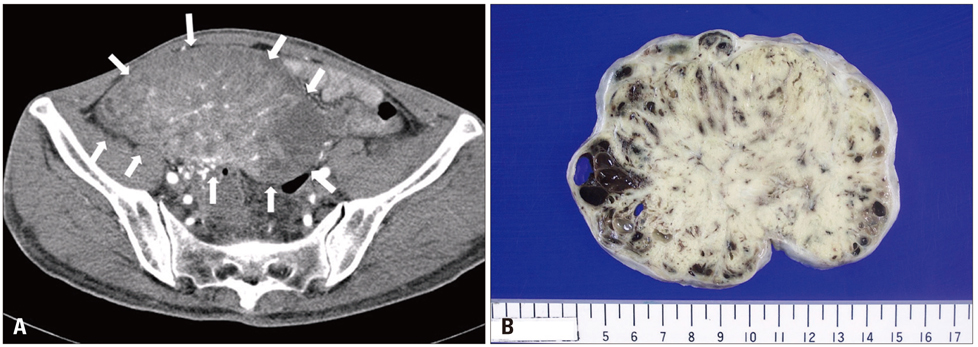
Fig. 3 Computed tomographic findings of carcinoid tumor. A large mass with inhomogenous density occupies the right pelvic cavity. The mass (white arrow) consists of multiple thick-enhancing septa and enhancing central soft tissue density (A). The right ovary is grossly enlarged; it is measured to be 80 × 124 × 78 mm in size and to weigh 461 g. The ovarian surface is smooth. The cut surface of the mass is bright yellow and solid, and it shows several foci of hemorrhage (B).
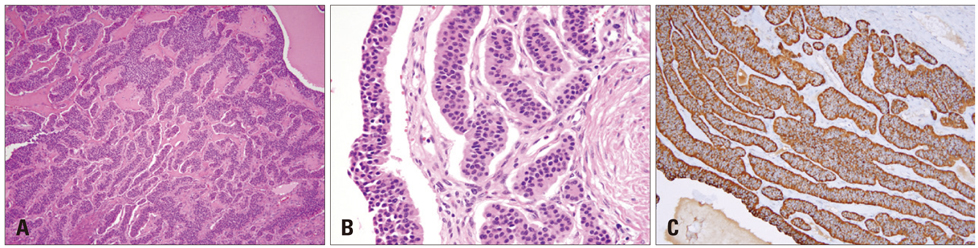
Fig. 4 Microscopic appearance of ovarian carcinoid tumor. Photomicrograph showing solid nests and broad trabeculae of tumor by cellular proliferation. These patterns were lined with one to two layers of cells (hematoxylin-eosin, 100×) (A). The regular round tumor cells have uniform rounded nuclei and abundant fibrovascular stroma (hematoxylin-eosin, 400×) (B). Immnuohistochemistry stains for neuroendocrine marker of the tumor cells reveals diffuse, strong, granular, and cytoplasmic staining (brown color) with chromogranin A (chromogranin, 100×) (C).
Reference
-
1. Modlin IM, Sandor A. An analysis of 8305 cases of carcinoid tumors. Cancer. 1997. 79:813–829.
Article2. Stephan E, de Wit J. Carcinoid heart disease from primary carcinoid tumour of the ovary. Haemodynamic and cine coronary angiocardiographic study after operation. Br Heart J. 1974. 36:613–616.
Article3. Chaowalit N, Connolly HM, Schaff HV, Webb MJ, Pellikka PA. Carcinoid heart disease associated with primary ovarian carcinoid tumor. Am J Cardiol. 2004. 93:1314–1315.
Article4. Artaza A, Beiner JA, Gonzalez M, Aranda I, de Teresa EG, Pulpon LA. Carcinoid heart disease: report of a case secondary to a pure carcinoid tumour of the ovary. Eur Heart J. 1985. 6:800–805.
Article5. Simula DV, Edwards WD, Tazelaar HD, Connolly HM, Schaff HV. Surgical pathology of carcinoid heart disease: a study of 139 valves from 75 patients spanning 20 years. Mayo Clin Proc. 2002. 77:139–147.
Article6. Blick DR, Zoghbi WA, Lawrie GM, Verani MS. Carcinoid heart disease presenting as right-to-left shunt and congestive heart failure: successful surgical treatment. Am Heart J. 1988. 115:201–203.
Article7. Mansencal N, Mitry E, Forissier JF, Martin F, Redheuil A, Lepére C, Farcot JC, Joseph T, Lacombe P, Rougier P, Dubourg O. Assessment of patent foramen ovale in carcinoid heart disease. Am Heart J. 2006. 151:1129.e1–1129.e6.
Article8. Zuetenhorst JM, Bonfrer JM, Korse CM, Bakker R, van Tinteren H, Taal BG. Carcinoid heart disease: the role of urinary 5-hydroxyindoleacetic acid excretion and plasma levels of atrial natriuretic peptide, transforming growth factor-beta and fibroblast growth factor. Cancer. 2003. 97:1609–1615.9. Kim YJ, Sohn DW, Bang YJ, Oh BH, Choi YS, Lee YW. Myocardial Involvement of Carcinoid Heart Disease: A Case Report. J Korean Soc Echocardiogr. 1998. 6:95–99.
Article10. Lundin L, Norheim I, Landelius J, Oberg K, Theodorsson-Norheim E. Carcinoid heart disease: relationship of circulating vasoactive substances to ultrasound-detectable cardiac abnormalities. Circulation. 1988. 77:264–269.
Article11. Møller JE, Connolly HM, Rubin J, Seward JB, Modesto K, Pellikka PA. Factors associated with progression of carcinoid heart disease. N Engl J Med. 2003. 348:1005–1015.
Article12. Møller JE, Pellikka PA, Bernheim AM, Schaff HV, Rubin J, Connolly HM. Prognosis of carcinoid heart disease: analysis of 200 cases over two decades. Circulation. 2005. 112:3320–3327.13. Connolly HM, Pellikka PA. Carcinoid heart disease. Curr Cardiol Rep. 2006. 8:96–101.
Article14. Pellikka PA, Tajik AJ, Khandheria BK, Seward JB, Callahan JA, Pitot HC, Kvols LK. Carcinoid heart disease. Clinical and echocardiographic spectrum in 74 patients. Circulation. 1993. 87:1188–1196.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Carcinoid Heart Disease: A Rare Cause of Right Ventricular Dysfunction Evaluation by Transthoracic 2D, Doppler and 3-D Echocardiography
- Isolated Tricuspid Regurgitation Caused by Annular Dilatation
- Improvement of Severe Tricuspid Regurgitation with Right Heart Failure Associated with Thyrotoxicosis due to Graves' Disease
- Reversible severe tricuspid regurgitation with right heart failure associated with thyrotoxicosis
- Tricuspid Regurgitation in Heart Diseases in Infants and Children
